
Translate this page into:
Demographic profile and spectrum of ultrasonographic findings in medial knee pain: An observational study

-
Received: ,
Accepted: ,
How to cite this article: Joshi AD, Gupta S, Gaur AK, Mhambre AS, Shukla A. Demographic profile and spectrum of ultrasonographic findings in medial knee pain: An observational study. Indian J Med Sci 2020;72(3):201-5.
Abstract
Objectives:
Medial knee pain is a common occurrence in people of various age groups with different conditions involving underlying structures. Ultrasound is used in assessing various complex knee pathologies as relying solely on clinical evaluation can be difficult. There are hardly any studies showing the compartmental analysis of knee pain using ultrasound. This study analyses the demographic profile and associated various ultrasonographic findings in patients with medial knee pain.
Material and Methods:
A cross-sectional study was done with participants of age 18 and above with medial knee pain. Screening was done by a Physical Medicine and Rehabilitation specialist in outpatient department and the ultrasonographic evaluation by a radiologist. Demographic profile and ultrasonographic findings of 46 participants were documented and studied.
Results:
Out of 46 participants studied, 95.65% were females. The mean age of distribution was 50.61 years and 52% of participants were overweight and 33% with obesity Class-I. Ultrasonography revealed abnormality of medial collateral ligament (45.65%), pes anserine tendon (41.30%) and bursa (4.55%), medial meniscus (36.96%), joint effusion (54.35%), and synovial hypertrophy, Baker’s cyst, and osteophytes.
Conclusion:
Older age, female gender, and increased body mass index are likely associated with medial knee pain with variable underlying conditions. These conditions can be differentiated with use of ultrasound by visualizing the abnormalities in underlying anatomical structures. Ultrasonography can be used with adequate knowledge and experience as a guide and tool in optimal management of wide spectrum of knee problems.
Keywords
Medial knee pain
Ultrasonography
Musculoskeletal problem

INTRODUCTION
Knee pain accounts for approximately one-third of the musculoskeletal problems seen in the primary care setting.[1] It is a common entity seen in sports medicine practice and geriatric population. Pain in the medial compartment of the knee is a common occurrence in people of various age groups and different gender. The differential diagnosis for medial knee pain includes medial collateral ligament sprain, medial compartment degenerative joint disease, medial meniscal tear, pes anserine bursitis, or medial plica syndrome.[2] Knee being a complex structure with challenging clinical evaluation, even the most experienced clinical staff using the strictest of clinical methods are not always enough to diagnose the cause.[3] Musculoskeletal ultrasound is useful for diagnosing a variety of regional pain syndromes and soft-tissue rheumatism.[4] It is viewed as an extension of our physical examination with advantage of dynamic assessment and easy availability.[5] There are hardly any studies done showing knee pain analysis according to the compartment involved and use of ultrasonography for the same. The objective of this study is to analyze the demographic profile of patients with medial knee pain visiting a rehabilitation setting and assess the various ultrasound findings associated with it.
MATERIAL AND METHODS
It is a cross-sectional observational study done in outpatient department (OPD) setting of Physical Medicine and Rehabilitation Department. The STROBE cross-sectional reporting guidelines were used by the authors for this study.[6] The ethical approval was waived off as the data were obtained without additional intervention or monitoring procedure for data collection. Patients of age 18 and above reporting in OPD for first time with complaints of medial knee pain were screened by a Physical Medicine and Rehabilitation specialist. Considering the complexity of knee pathologies and variety of presentations, patients with history of the previous treatment for knee pain and knee pain other than or in addition to medial compartment were excluded from the study. The data were collected over a period of 5 weeks in a total of 15 OPD settings (3 OPD/week). The data of demographic details comprised age, sex, body weight, height, and number of involved knees.
Selected individuals underwent ultrasonographic evaluation after written informed consent. It was done by a radiologist experienced with musculoskeletal ultrasound practice. Ultrasonographic findings of the medial knee joint structures were recorded which comprised medial collateral ligament, medial joint line and surface, pes anserinus tendon and bursa, medial meniscus, suprapatellar recess (medial), and medial (semimembranosus and medial gastrocnemius) knee bursae.[7] The linear array transducer of the Siemens Acuson NX3 ultrasound machine (California, USA) with frequency of 7–12 MHz was used for the assessment.
RESULTS
Study comprised 46 participants with evaluation of 67 knees. Categorical variables were presented in number and percentage, and continuous variables were presented as mean ± SD and median. Normality of data was tested by Kolmogorov–Smirnov test. If the normality was rejected, then non-parametric test was used. The data were entered into MS EXCEL spreadsheet and analysis was performed using Statistical Package for the Social Sciences version 21.0. In this study, mean age of presentation was 50.61 years ranging from 22 years to 75 years with standard deviation of ± 10.65 [Figure 1a]. Out of 46 patients, 44 were females (95.65%) and two were males (4.35%). Bilateral involvement was seen in 21 patients (45.65%) and unilateral involvement comprised 54.34% of total. In unilateral presentation, the right knee (41.30%) was more involved [Table 1].
| Frequency | Percentage | |
|---|---|---|
| Gender | ||
| Male | 02 | 4.35 |
| Female | 44 | 95.65 |
| Side involved | ||
| Both | 21 | 45.65 |
| Left | 06 | 13.04 |
| Right | 19 | 41.30 |
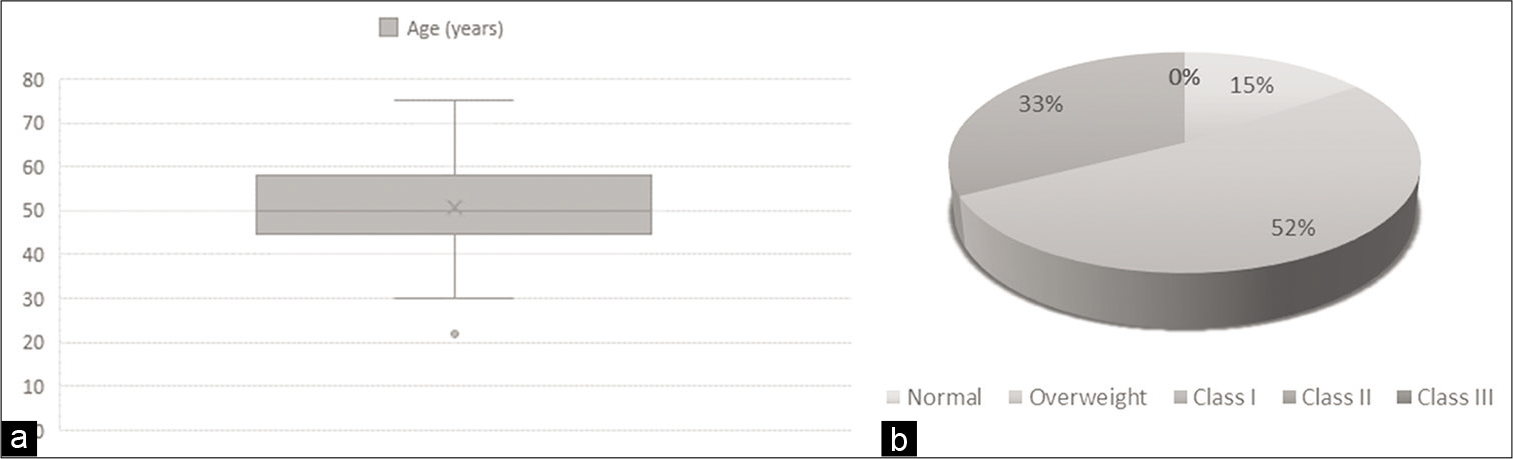
- (a) Distribution of age in study participants. (b) Categorization of body mass index.
Body mass index classification was done using World Health Organization international classification.[8] There were seven participants with normal body mass index (18.5–24.9 kg/m2), 24 participants being overweight (25–29.9 kg/m2) and 15 participants with Class I obesity (30–34.9 kg/m2). No participant belonged to Classes II and III of obesity in this study [Figure 1b].
The ultrasonography was performed, and abnormal findings of the underlying structures were documented [Table 2].
| Ultrasonographic findings | Normal (%) | Abnormal (%) | Total |
|---|---|---|---|
| Pes anserine bursa | 44 (95.45) | 2 (4.55) | 46 |
| Pes anserine tendon | 27 (58.70) | 19 (41.30) | 46 |
| Medial collateral ligament | 25 (54.35) | 21 (45.65) | 46 |
| Medial meniscus | 29 (63.04) | 17 (36.96) | 46 |
| Effusion | 21 (45.65) | 25 (54.35) | 46 |
| Other findings (osteophytes, synovial hypertrophy, Baker’s cyst, etc.) | 36 (82.61) | 8 (17.39) | 46 |
Imaging of the pes anserine bursa showed abnormality in two participants (4.35%) with findings of focal linear to oval fluid collection deep to the pes anserinus tendon [Figure 2a], whereas imaging of the pes anserinus tendon showed abnormality in total of 27 participants (58.70%) with findings of linear hypo-echogenicity and loss of normal fibrillar compact echo-pattern of the pes anserine tendon and occasional fluid tracking along the tendon suggestive of tendonitis [Figure 2b and c].

- (a) Fluid (box) in pes anserinus bursa. (b) Pes anserinus tendon with altered echogenicity (arrow) and fluid tracking. (c) Pes anserinus tendon with altered echogenicity (arrow).
Abnormality along with medial collateral ligament was noted in 21 participants (45.65%) with findings of focal hypoechogenicity suggestive of injury of the ligament [Figure 3a]. Some cases also showed medial displacement.
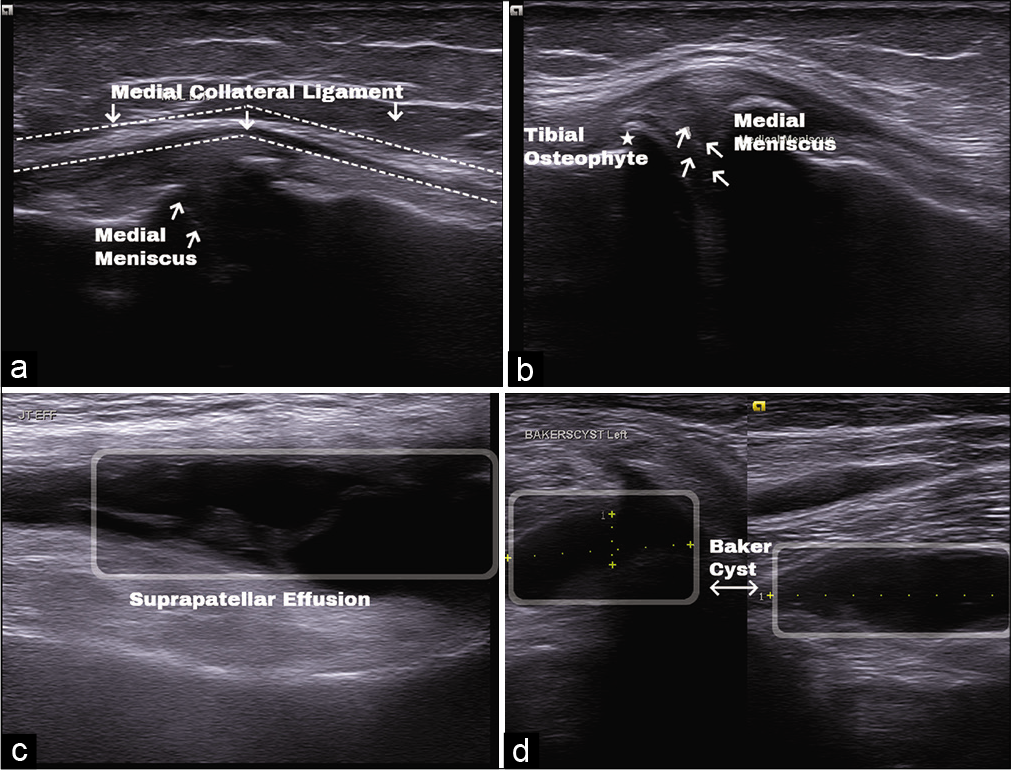
- (a) Medial collateral ligament (dotted line) altered echogenicity with medial displacement and protrusion of medial meniscus (arrow). (b) Protrusion of body medial meniscus (arrow) and tibial osteophyte (star). (c) Joint effusion in suprapatellar recess (box). (d) Baker cyst (box) with short and long axis view.
On imaging medial meniscus showed protrusion/extrusion of body of the medial meniscus beyond the bony joint line suggestive of degeneration or tear [Figure 3a and b]. The findings were limited to a total of 17 patients (36.96%). One patient reported to have anechoic cleft in anterior horn suggestive of tear.
Almost 25 of the total participants (54.35%) were reported to have suprapatellar effusion suggested by anechoic or hypoechoic distention of the suprapatellar recess [Figure 3c]. Quantification of the fluid was not done.
There were eight participants (17.89%) who were reported with findings such as osteophytes in medial compartment of knee joint [Figure 3b] or synovial hypertrophy or Baker’s cyst [Figure 3d]. As the findings were not attributable to a single anatomical structure, they were categorized into other findings.
DISCUSSION
In this study, we evaluated 46 participants with the mean age of presentation of 50.61 years with standard deviation of ±10.65. Loeser in his study mentioned age related changes in musculoskeletal system affecting the joint tissues and function making joint more susceptible to damage.[9] With the mean age 50.61 years, the patients in this study show age as the important contributory factor for pain irrespective of external or mechanical stimuli.
In addition to age, the data showed 95.65% female participants with medial knee pain. This is supported by Leveille et al. with findings of more prevalence and widespread musculoskeletal pain in older women than men.[10]
Through body mass index analysis of the subjects, we found that majority belonged to overweight (52%) or obesity Class I (33%) than normal body mass index (15%). Calenzani et al. mentioned the high prevalence of musculoskeletal pain and limitation in activities due to pain in obese individuals which supports the study finding.[11] They also observed activity limitation due to pain in regions of knees and/or ankles, feet, and lower back in the obese patients.
We had some young adults in this study with propensity for obesity indicating future risk of functional limitation as per Frilander et al., who stated that development of severe obesity over life course increased the risk of knee pain by 80% and functional limitation by 93%.[12]
The mean age of 50.61 years, female preponderance and propensity for obesity in the studied population makes them likely candidate for future osteoarthritis of knee with pain. Silverwood et al., in a systematic review on risk factors for knee osteoarthritis in older adults found that the main factors associated with onset of knee pain were being overweight, obesity, and female gender.[13]
The ultrasonography was chosen as to visualize the soft structures in the knee as it was non-invasive and was possible to be done in one sitting without any prior preparation.
The ultrasonography of the pes anserine bursa showed focal linear to oval fluid collection deep to the pes anserinus tendon (4.55%) and the pes anserinus tendon showed linear hypo-echogenicity and loss of normal fibrillar compact echo-pattern with occasional fluid tracking along the tendon (41.30%). Similar findings are given by Alves et al. in pathologic conditions in ultrasound of medial knee compartment.[14] Clinical differentiation between primary tendon and primary bursal pain can be challenging.[15] With the results in the study, it can be said that ultrasound can be helpful in such differentiation.
Medial collateral ligament abnormality with hypoechogenicity and/or displacement has been noted in 21 patients. Homogenous and thin compact fibrillar appearance of medial collateral ligament are considered as normal and heterogeneous hypo-echogenic and thickened appearance as abnormal in the study conducted by Lee et al.[16] Alves et al. mentioned regarding loss of the normal taut fibrillar structure of medial collateral ligament as injury in addition to the thickening and stresses on importance of ultrasound in grading the ligament injury with dynamic assessment.[14] In this study, the thickness was not quantified, nor the dynamic assessment was done but the altered structural pattern was marked as an abnormality which is supported in both the studies mentioned.
Medial meniscus showed protrusion/extrusion of body and/ or hypoechoic area suggestive of either tear or degenerative change in 17 patients (36.96%) with only one finding of anechoic cleft in anterior horn suggestive of tear. This was consistent with findings of Alves et al. who mentioned the tears as focal hypoechoic or anechoic defects and degeneration as heterogenicity of body with extrusion and fragmentation.[14] Although helpful it should be considered as a screening part in suspected meniscal injuries, as the magnetic resonance imaging is more sensitive in detecting and determining the type of meniscal lesions completely.[17]
Almost 25 participants (54.35%) have showed suprapatellar effusion in this study characterized by anechoic or hypoechoic distention of the suprapatellar recess. Even a small joint effusion can be found in an extended knee in medial or lateral recess.[7,14] As supported by Alves et al., the differentiation cannot be done between septic and aseptic effusion, but ultrasound can be used in documentation and guidance for aspiration of the effusion when needed.[14]
Other findings which were reported in our study were Baker cyst, synovial hyperplasia, and changes of osteoarthritis in knee like the presence of osteophytes. Baker’s cyst also known as popliteal cyst is distension of semimembranosusmedial gastrocnemius bursa[2,7,14] and should be looked for while considering potential cause of medial knee pain.
The ultrasonography aids in better clinic-radiological correlation. Because of the easy availability, outpatient set up and no specific preparatory requirements for the patient, it can be used to localize the pathology correlating with the symptoms. This spectrum of ultrasonographic findings can be used to correlate the causes of medial knee pain as seen in adults with overuse syndrome, traumatic causes, and age-related degenerative conditions, mentioned by Calmbach and Hutchens as differential diagnosis of knee pain.[2]
This study throws light on the diagnostic utility of ultrasound. However, ultrasound is considered the tool not only for diagnostic efficacy but also therapeutic accuracy. With appropriate knowledge and experience, ultrasound has shown to increase accuracy of not only corticosteroid injection into joint cavity, bursa, and tendon sheath but also it is popularly used method for regional nerve block or focal spasticity management.[5]
Although ultrasonography is gaining popularity in the management of musculoskeletal problems, its usefulness is limited to some extent. The primary limitation lies with operator dependency and requirement of training and experience for accurate image acquisition and interpretation.[13]
Magnetic resonance imaging turns out to be the modality of choice for pathology involving deep structures, intraarticular lesions, infections, or even tumorous conditions.[18] For knee, ultrasonography is of limited use for the assessment of cruciate ligaments, articular cartilage, joint surface, bone marrow, or intramedullary lesion where magnetic resonance imaging gives better results.[13]
We understand the limitations of our analysis with this convenience sampling. Smaller sample size is the limitation in our study but it has been supported by the findings that were standardized and had no inter-examiner biases when it came to the undertaking the patient as well as radiologist performing the ultrasonography.
Our research design does not allow for any true hypothesis testing due to its small sample size, but results suggest further studying. The study suggests that the knee conditions should be studied more separately as per the site of pain or compartments with possible clinical correlation.
CONCLUSION
The present study highlights the demographic profile of patients with medial knee pain and role of ultrasound in the evaluation. Older age, female gender, and increased body mass index are likely associated with medial knee pain with variable underlying conditions. Ultrasonography helps in differentiation of these conditions and establishing diagnosis by visualization of the abnormalities in composition of underlying anatomical structures. With adequate knowledge, experience and standardized findings, ultrasonography will serve as a guide and tool in optimal management of wide spectrum of problems in knee.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Evaluation of patients presenting with knee pain: Part I. History, physical examination, radiographs, and laboratory tests. Am Fam Physician. 2003;68:907-12.
- [Google Scholar]
- Evaluation of patients presenting with knee pain: Part II. Differential diagnosis. Am Fam Physician. 2003;68:917-22.
- [Google Scholar]
- Correlation between ultrasonographic findings and the response to corticosteroid injection in pes anserinus tendinobursitis syndrome in knee osteoarthritis patients. J Korean Med Sci. 2005;20:109-12.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic accuracy of ultrasonography in evaluation of knee injuries with magnetic resonance imaging correlation. Int J Anat Radiol Surg. 2018;7:RO50-5.
- [Google Scholar]
- Diagnostic ultrasound In: Frontera WR, DeLisa JA, Gans BM, Walsh NE, Robinson LR, Basford JR, eds. DeLisa's Physical Medicine & Rehabilitation Principles and Practice (5th ed). Philadelphia, PA: Wolters Kluwer; 2010. p. :211.
- [Google Scholar]
- The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int J Surg. 2014;12:1495-9.
- [CrossRef] [PubMed] [Google Scholar]
- Knee ultrasound. In: Fundamentals of Musculoskeletal Ultrasound (2nd ed). Philadelphia, PA: Elsevier; 2013. p. :212-56.
- [CrossRef] [Google Scholar]
- Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157-63.
- [CrossRef] [Google Scholar]
- Age-related changes in the musculoskeletal system and the development of osteoarthritis. Clin Geriatr Med. 2010;26:371-86.
- [CrossRef] [PubMed] [Google Scholar]
- Sex differences in musculoskeletal pain in older adults. Pain. 2005;116:332-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of musculoskeletal symptoms in obese patients candidates for bariatric surgery and its impact on health related quality of life. Arch Endocrinol Metab. 2017;61:319-25.
- [CrossRef] [PubMed] [Google Scholar]
- Obesity in early adulthood predicts knee pain and walking difficulties among men: A life course study. Eur J Pain. 2016;20:1278-87.
- [CrossRef] [PubMed] [Google Scholar]
- Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthritis Cartilage. 2015;23:507-15.
- [CrossRef] [PubMed] [Google Scholar]
- US of the knee: Scanning Techniques, pitfalls, and pathologic conditions. Radiographics. 2016;36:1759-75.
- [CrossRef] [PubMed] [Google Scholar]
- Musculoskeletal disorders of the lower limb In: Cifu DX, ed. Braddom's Physical Medicine and Rehabilitation (5th ed). Philadelphia, PA: Elsevier; 2016. p. :785.
- [Google Scholar]
- Medial collateral ligament injuries of the knee: Ultrasonographic findings. J Ultrasound Med. 1996;15:621-5.
- [CrossRef] [PubMed] [Google Scholar]
- MRI versus ultrasound in diagnosis of meniscal tear in knee joint. Egypt J Hosp Med. 2019;74:303-9.
- [Google Scholar]
- Imaging techniques relative to rehabilitation In: Frontera WR, DeLisa JA, Gans BM, Walsh NE, Robinson LR, Basford JR, eds. DeLisa's Physical Medicine & Rehabilitation Principles and Practice (5th ed). Philadelphia, PA: Wolters Kluwer; 2010. p. :139-67.
- [Google Scholar]




