
Translate this page into:
Parenteral testosterone therapy’s effect on penile size before hypospadias surgery
-
Received: ,
Accepted: ,
How to cite this article: Godse S, Kumar A, Singh H, Choudhary G, Chhabra MK. Parenteral testosterone therapy’s effect on penile size before hypospadias surgery. Indian J Med Sci 2023;75:15-7.
Abstract
Objectives:
The purpose of this study was to see the effect of parenteral testosterone injection on penile length, glans diameter, and diameter at the base of the penis in hypospadias patients before surgery.
Material and Methods:
The study was conducted from September 2019 to March 2021. This study comprised a total of 20 hypospadias patients. At a dose of 2 mg/kg body weight, an injection testosterone propionate was administered deep intramuscularly in three doses with a 3-week gap before reconstructive surgery. Before surgery, the penile length, glans diameter, and penile diameter at the base of the penis were all measured.
Results:
The mean increase in penile length, glans diameter, and diameter at the base of penis following parenteral testosterone therapy was 1.07 ± 0.23 cm (P < 0.001), 1.01 ± 0.46 cm (P < 0.001), and 0.92 ± 0.12 cm (P < 0.001), respectively. All three measurements were statistically significant.
Conclusion:
Intramuscular testosterone increased penis size, glans diameter, and penile diameter without causing any notable side effects. Development of fine pubic hair, acne, and aggressiveness is minor adverse effects.
Keywords
Hypospadias
Testosterone
Glans penis

INTRODUCTION
Hypospadias is a birth defect that is associated with three anomalies of the penis
Opening of urethral orifice on ventral surface
Ventral curvature of the penis
Hypospadias is the most common congenital defect, which affects 0.3–0.7% of all live male births.[3]
Hypospadias is most likely caused by a combination of factors.[4]
The aim of hypospadias repair is to achieve excellent functional and cosmetic results.[5] Anthropometry of the penis particularly the biometrics of the glans penis is an important consideration before hypospadias repair.[6] Studies have shown that small glans diameter measuring <14 mm (mm) is associated with glans dehiscence following hypospadias repairs.[7,8] It has been hypothesized that increasing the size and girth of the penis preoperatively may lead to a larger surgical site, thus reducing intraoperative and postoperative complications of the hypospadias corrective surgery.
To enlarge phallus size, temporary stimulation with testosterone or dihydrotestosterone cream has been used. However, the results were inconsistent, but its absorption was also variable.[9] This observation has made surgeons administer parenteral testosterone to increase the glans diameter before hypospadias repair.[10,11] Testosterone is the peripherally acting androgen causing growth and development of the external genitalia and secondary sexual characters. The effect is more pronounced on the genitals as a result of higher expression of androgen receptors.
MATERIAL AND METHODS
This prospective study was conducted at the Department of Urology, Dr. S.N Medical College, Jodhpur, from September 2019 to March 2021. A total of 20 patients with hypospadias were included in this study of ages between 6 months and 18 years.
Inclusion criteria
Six months–18 years of male patients with hypospadias were included in the study.
Exclusion criteria
The following criteria were excluded from the study:
Patients for hypospadias reoperation
Undescended testis (unilateral or bilateral).
Informed consent was obtained from the patient’s caregivers.
Following parameters were measured in centimeters:
Stretched penile length from pubic bone to the tip of the glans
Maximum transverse diameter of the glans penis at the coronal sulcus
Diameter of penis at its base.
These dimensions were measured before the therapy and on the day of surgery using a Vernier caliper. At least two measurements of each parameter were made by the same person and the average was taken. This minimized observer and operator variability.
Injection testosterone propionate was given deep intramuscularly in three doses with an interval of 3 weeks before reconstructive surgery at the dose of 2 mg/kg body weight. Side effects such as the development of fine pubic hair, acne, and aggressive behavior as reported by parents were also evaluated.
IBM Statistical Package for the Social Sciences for Windows version 23 (IBM Corp., Armonk, NY) was used for data entry and analysis. Data were expressed as percentages, median, means, and standard deviation. The Chi-square test or Student’s t-test was used to test for significance. P < 0.05 was considered statistically significant.
RESULTS
Patient demographics
The mean age of presentation was 3.8 years (range, 6 months–10 years). Eight patients were between 6 months and 2 years of age. Six patients were between 2 and 5 years of age. Six patients were more than 5 years of age. Familial history was seen in two patients.
Type of hypospadias
Of 20 cases, 10 were of distal (three coronal, four subcoronal, and three distal penile), seven were of middle (five midshaft and two proximal penile), and three were of proximal hypospadias (three penoscrotal) [Figure 1].
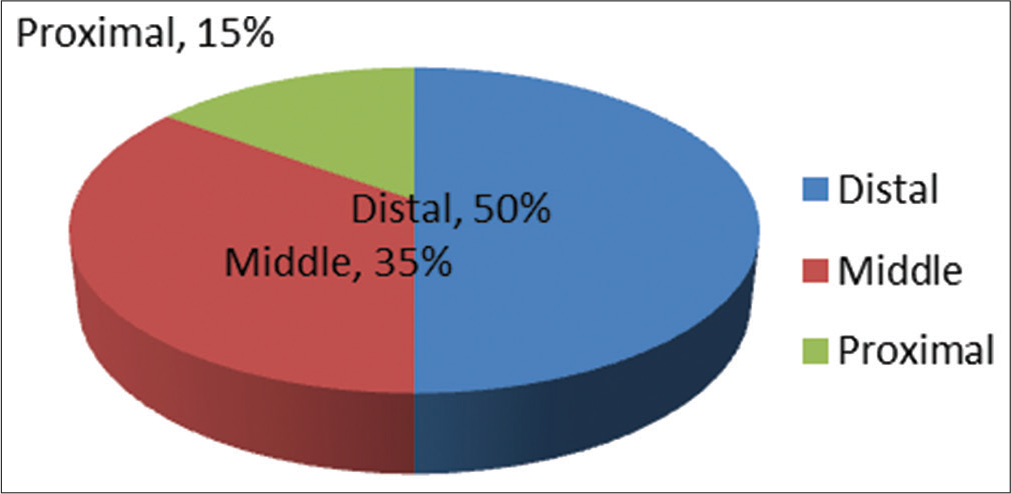
- Types of hypospadias.
Penile dimensions
The mean stretched penile length was 2.45 ± 0.82 cm. It increased to 3.52 ± 0.56 cm. The mean increase in penile length was 1.07 ± 0.23 cm (P < 0.001) [Table 1], [Figure 2].
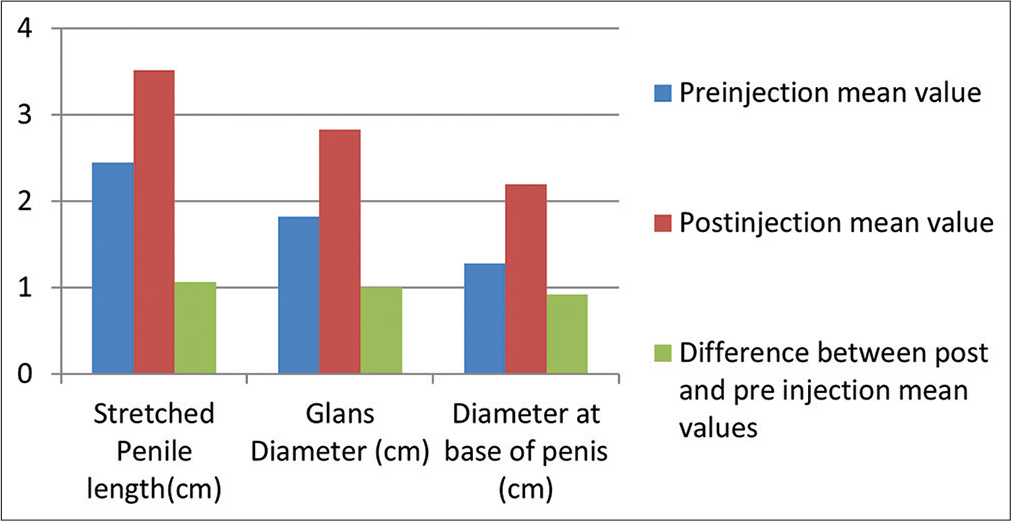
- Penile dimensions before and after testosterone injection.
| Mean values | Stretched penile length (cm) | Glans diameter (cm) | Diameter at base of penis (cm) |
|---|---|---|---|
| Pre-injection | 2.45±0.82 | 1.82±0.42 | 1.28±0.18 |
| Post-injection | 3.52±0.56 | 2.83±0.28 | 2.20±0.32 |
| Difference | 1.07±0.23 | 1.01±0.46 | 0.92±0.12 |
| P value | <0.001 | <0.001 | <0.001 |
The mean of transverse diameter of the glans was 1.82 ± 0.42 cm which increased to 2.83 ± 0.28 cm. The increase was statistically significant (P < 0.001).
The diameter at the base of penis was 1.28 ± 0.18 cm which increased to 2.20 ± 0.32 cm. The difference was statistically significant (P < 0.001).
Two patients developed mild pubic hair, after two doses of injection. There were no parents reported cases of acne or aggression.
DISCUSSION
Testosterone increases size of the penis in prepubertal males due to its androgenic effects. This effect is beneficial for the surgical repair of hypospadias because a larger penile size makes correction easier and less risky.[12]
One study that administered human chorionic gonadotropin (hCG) to children over 5 weeks found that hCG produces disproportionate penile enlargement and decreases the severity of hypospadias.[13] However, the use of hCG lacked a treatment protocol and there were wide variations in response.
Topical application of testosterone has also been found effective in increasing penile length and glans circumference.[14] The drawback of topical testosterone is that the results of its use are inconsistent due to variable absorption. Concerns over absorption and potential side effects after local application led to the use of injectable slowly releasing testosterone for pre-operative genital stimulation.
In a study conducted by Ahmad et al., 23 patients aged between 6 months and 10 years; preoperatively, testosterone was given deep intramuscularly in three doses at 4, 3, and 2 weeks before reconstructive surgery at the dose of 2 mg/kg body weight and concluded that parenteral testosterone can be safely used to improve the surgical outcome of hypospadias repair.[15]
In our study, the effect of intramuscular testosterone on penile growth from the day of injection to the day of operation was statistically significant (P < 0.001). The mean increase in penile length was 1.07 ± 0.23 cm. There was an increase in transverse glans diameter of 1.01 ± 0.46 [Table 1]. The texture and vascularity of penile skin also improved. This increased transverse length is helpful particularly in proximal hypospadias. Negligible side effects were noted in the form of development of pubic hair in two patients.
CONCLUSION
Penile augmentation with parenteral testosterone is associated with an increase in phallus size and diameter with few adverse effects. The vascularity of penile skin also improved. Thus, parenteral testosterone can be safely used to improve the results of hypospadias surgery.
Limitation
Study lacked a control group and there was no follow-up of patients post-surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Genetic pathway of external genitalia formation and molecular etiology of hypospadias. J Pediatr Urol. 2010;6:346-54.
- [CrossRef] [PubMed] [Google Scholar]
- Hypospadias: Anatomy, etiology, and technique. J Pediatr Surg. 2006;41:463-72.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of the effect of urethral plate width on outcome of hypospadias repair. J Pediatr Urol. 2019;15:627-e6.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric penile and glans anthropometry nonograms: An aid in hypospadias management. J Indian Assoc Pediatr Surg. 2017;22:9-12.
- [CrossRef] [PubMed] [Google Scholar]
- Glans penis width in patients with hypospadias compared to healthy controls. J Pediatr Urol. 2013;8:1188-91.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of risk factors for glans dehiscence after tubularized incised plate hypospadias repair. J Urol. 2011;185:1845-9.
- [CrossRef] [PubMed] [Google Scholar]
- Testosterone therapy in microphallic hypospadias: Topical or parenteral? J Pediatr Surg. 2003;38:221-3.
- [CrossRef] [PubMed] [Google Scholar]
- Use of parenteral testosterone prior to hypospadias surgery. Pediatr Surg Int. 2003;19:82-4.
- [CrossRef] [PubMed] [Google Scholar]
- Dehydrotestosterone penile stimulation in hypospadias surgery. Eur Urol. 1982;8:201-3.
- [CrossRef] [PubMed] [Google Scholar]
- The efficacy of dihydrotestosterone transdermal gel before primary hypospadias surgery: A prospective, controlled, randomized study. J Urol. 2008;179:684-8.
- [CrossRef] [PubMed] [Google Scholar]
- Microphallic hypospadias-the use of human chorionic gonadotropin and testosterone before surgical repair. J Urol. 1999;162:1440-1.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of topical versus parenteral testosterone in children with microphallic hypospadias. Pediatr Surg Int. 2009;25:57-9.
- [CrossRef] [PubMed] [Google Scholar]
- Role of parenteral testosterone in hypospadias: A study from a teaching hospital in India. Urol Ann. 2011;3:138-40.
- [CrossRef] [PubMed] [Google Scholar]




