
Translate this page into:
Incidence of cancer in a rural registry in India-Ratnagiri, Maharashtra
*Corresponding author: Ganesh Balasubramaniam, Biostatistics and Epidemiology, Centre for Cancer Epidemiology, Advanced Centre for Treatment, Research and Education in Cancer, Tata Memorial Centre, Navi Mumbai, Maharashtra, India. drbganeshtmh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Balasubramaniam G, Cheulkar SA, Joshi PK, Patil AR, Badwe R, Dikshit R, et al. Incidence of cancer in a rural registry in India-Ratnagiri, Maharashtra. Indian J Med Sci 2023;75:47-52.
Abstract
Objectives:
The objective of this study was to elucidate the various challenges in establishing cancer registry and further provide inputs to commission infrastructure for cancer treatment, in this rural setup.
Materials and Methods:
Population of Ratnagiri district is covered in its entirety. Registry data for the year 2015 - 2016 is analyzed. Population-Based Cancer Registry staff has visited various hospitals, pathology laboratories, radiological centers, panchayats, local physicians, anganwadi, primary health-care centers, etc., to collect the information. An in-house software was developed in visual basic with DB platform for data entry, validation checks and MS-Office Excel and SPSS Ver 21 were used for analysis.
Results:
Cancer incidence rate (age-adjusted incidence rate ) of Ratnagiri district is 39.1 and 39.6/100,000 for male and female, respectively, and is in comparison with other rural Indian registries. In males, mouth cancer and breast cancer in females were leading site of cancer.
Conclusion:
Results of Ratnagiri registry are valuable for cancer control activities.
Keywords
Cancer registry
Ratnagiri
Cancer incidence rate

INTRODUCTION
Cancer is one of the important causes of morbidity and mortality in India. Globally, out of 14 million, 1 million cancers were from India. Similarly, of 8 million cancer deaths worldwide, 0.7 million occurred in India.[1]
As cancer registries are vital for measuring disease burden, Indian Council of Medical Research, setup 36 Population-Based Cancer Registries (PBCRs) in India.[2] Tata Memorial Center (TMC) being a Premier Cancer Center in India, collaborated with B.K.L. Walawalkar Hospital, Dervan, Chiplun to setup the PBCR in this rural district.
According to 2011 Census data, the district total population is 1,615,069. The population density is 197 persons per sq. km and sex ratio of 1122 females per 1000 males in the District, showing female predominance.[3] There are nine talukas in Ratnagiri district, namely, Mandangad, Dapoli, Khed, Chiplun, Guhagar, Sangameshwar, Ratnagiri, Lanja, and Rajapur. The paper outlines the cancer incidence/mortality in Ratnagiri district of Maharashtra.
MATERIALS AND METHODS
PBCR collects data on all new cancer cases registered in defined geographical area. Before setting up the registry, a survey was done in Ratnagiri district. Due to hilly areas, access within Ratnagiri district is not easy. Training is provided to the registry staff to understand the medical terminologies, ways to approach the various sources to collect the information, etc.
Sources
The investigator visits various sources to collect the information of cancer patients. The sources include hospitals, pathology laboratories, radiological centers, villages, panchayats, local physicians, anganwadi, primary health-care centers, and NGOs. The cases who are residents of Ratnagiri mostly visit Tata Memorial Hospital (TMH), Mumbai and B.K.L Walawalkar Hospital, Dervan for diagnosis, treatment and follow-up.
Inclusion criteria
Only malignant cases are included in the study. The criteria being that the patient must be resident of Ratnagiri district for at least 1 year, residence confirmation is done by house visits or through telephone number. Once the required criteria is fulfilled, the desired information is collected such as demographic information, date of diagnosis, most valid basis of diagnosis, tumor site, and morphology and mortality details if the patient is dead.
Cancer reporting system
All cancer cases are coded as per International Classification of Diseases for Oncology – 3rd Ed. (ICD-O-3)[4] and ICD-10[5] guidelines provided by the World Health Organization publication ICD-O-3 which is dual classification for both topography and morphology.
Quality checks and duplicate checks
Multiple recordings of cancer cases from different sources are matched to register single case except for multiple primaries. Duplicates are excluded after matching name, age, sex, address, and site of cancer. There are two methods to find out duplicates. (1) An alphabetic index cards are maintained at registry office which contains registration number, name, sex, address, age, and site of cancer. Information obtained from any source is first checked into the existing index cards. If the index card already exist for the patient, then information is updated against the same registration number in the database, if not then new index card is filled up and new registration number is generated. (2) In-house software is developed for data entry. When the new case is entered into the system, the name is checked into the database for duplicate entry. If the name already exists, then registration number is listed to avoid the duplications. If not duplicate, new registration number is generated after checking the address, age, sex, and site of the patient.
Once the entry is completed for a particular year, the analysis is done in SPSS[6] software for generating tables. An in-house software was developed in visual basic with DB platform for data entry, validation checks and MS-Office Excel and SPSS Ver 21 were used for analysis.
RESULTS
The population of Ratnagiri District for the year 2015– 16 is computed using exponential growth rate between census population of 2001 and 2011.[7] The total population of Ratnagiri District is 1,577,041 for the year 2015–16. [Figure 1] shows the percentage distribution of estimated population of Ratnagiri district for the year 2015–16, based on 2001 and 2011 census population.
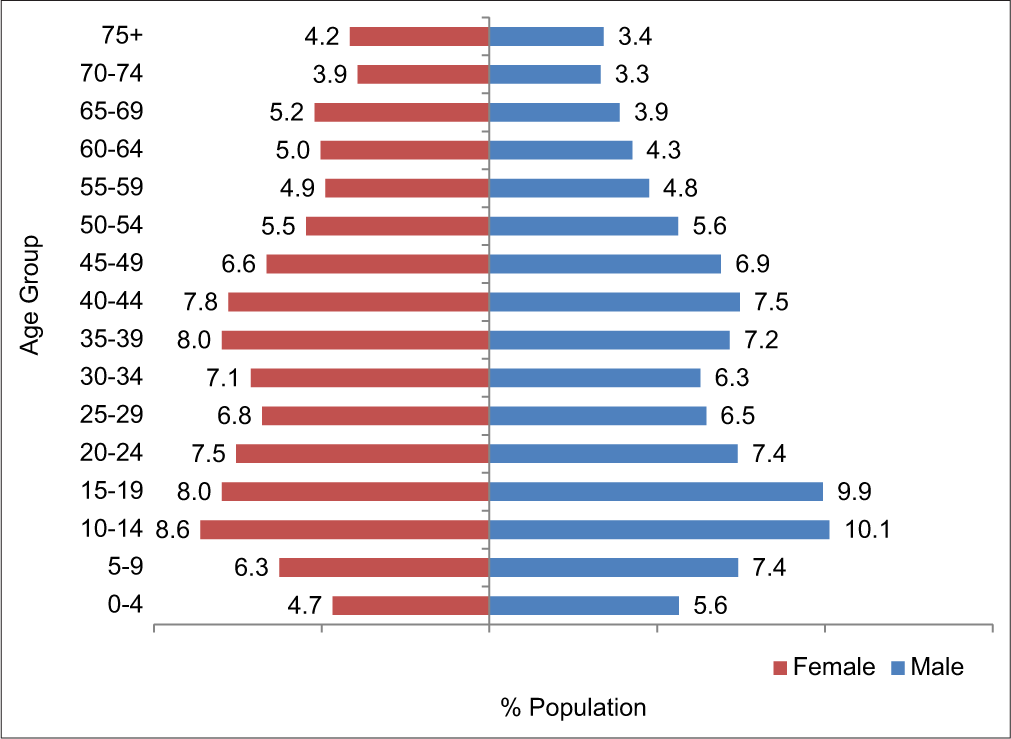
- Percentage distribution of estimated population of Ratnagiri district for the year 2015–2016, based on 2001 and 2011 census population.
According to Ratnagiri Registry Report 2015–16, the leading sites of cancer in Ratnagiri district are shown in [Table 1].[7] In males, mouth cancer and breast cancer in females were leading site of cancer.
| Male | Female | ||
|---|---|---|---|
| Site | AAR | Site | AAR |
| Mouth | 7.0 | Breast | 11 |
| Tongue | 2.9 | Mouth | 4.0 |
| NHL | 2.4 | Cervix | 3.0 |
| Esophagus | 1.9 | Ovary etc. | 2.8 |
| Lung | 1.8 | Esophagus | 2.2 |
| all sites | 39.1 | All sites | 39.6 |
[Table 2] shows the comparison of cumulative risk of developing cancer in 0–74 years of age in Ratnagiri District with other selected registries in India. One in every 25 males and one in every 24 females are likely to develop the cancer in 0–74 years of age in Ratnagiri district, indicating higher risk in female than male. Furthermore, the risk is much lower than other specified registries.
| Registry | One in number | |
|---|---|---|
| Male | Female | |
| Ratnagiri | 1 in 25 | 1 in 24 |
| Mumbai | 1 in 9 | 1 in 8 |
| Barshi Rural | 1 in 17 | 1 in 15 |
| Chennai | 1 in 8 | 1 in 7 |
[Table 3] shows the tobacco-related cancers in Ratnagiri for the year 2015–16. Nearly 65% of cancers in male and 38% in female are related to the tobacco-related cancer sites. Furthermore, oral cavity contributes around 19% of all cancers.[7]
| Site | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Oral cavity | 179 | 25.6 | 117 | 13.3 | 296 | 18.8 |
| Oropharynx | 19 | 2.7 | 10 | 1.1 | 29 | 1.8 |
| Nasopharynx | 5 | 0.7 | 2 | 0.2 | 7 | 0.4 |
| Hypopharynx | 29 | 4.1 | 11 | 1.3 | 40 | 2.5 |
| Larynx | 13 | 1.9 | 8 | 0.9 | 21 | 1.3 |
| Lung | 33 | 4.7 | 21 | 2.4 | 54 | 3.4 |
| Esophagus | 36 | 5.2 | 52 | 5.9 | 88 | 5.6 |
| Stomach | 30 | 4.3 | 26 | 3.0 | 56 | 3.6 |
| Gall bladder | 6 | 0.9 | 10 | 1.1 | 16 | 1.0 |
| Liver | 16 | 2.3 | 12 | 1.4 | 28 | 1.8 |
| Pancreas | 5 | 0.7 | 13 | 1.5 | 18 | 1.1 |
| Colon | 21 | 3.0 | 13 | 1.5 | 34 | 2.2 |
| Rectum | 20 | 2.9 | 18 | 2.1 | 38 | 2.4 |
| Kidney | 11 | 1.6 | 5 | 0.6 | 16 | 1.0 |
| Renal pelvis | 0.0 | 1 | 0.1 | 1 | 0.1 | |
| Urinary bladder | 12 | 1.7 | 5 | 0.6 | 17 | 1.1 |
| Myeloid leukemia | 13 | 1.9 | 9 | 1.0 | 22 | 1.4 |
| Total TRC | 448 | 64.1 | 333 | 37.9 | 781 | 49.5 |
| Other carcinomas | 251 | 35.9 | 545 | 62.1 | 796 | 50.5 |
| Total | 699 | 100.0 | 878 | 100.0 | 1577 | 100.0 |
[Figure 2] shows the various diagnosis methods used for diagnosis of cancer in Ratnagiri registry.
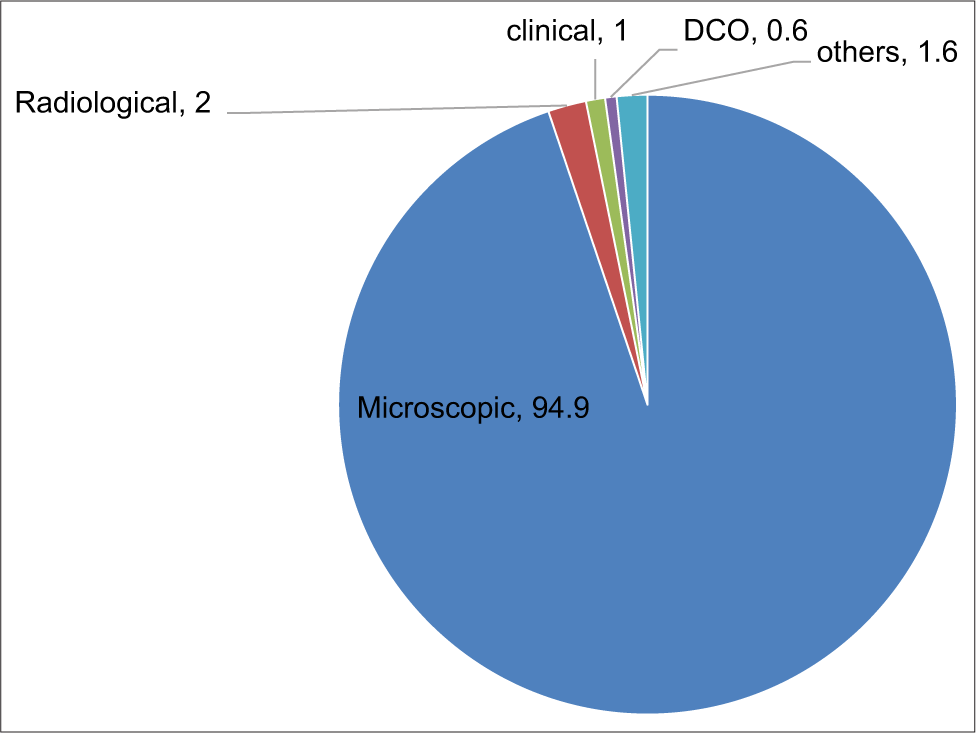
- Distribution of cancer cases by different methods of diagnosis. Year 2015–2016.
Around 95% of total cancer cases are diagnosed microscopically, 2.0% diagnosed on radiological grounds, 1.0% diagnosed clinically, 0.6% are included on the death certificate, and 1.6% cases are included from hospital record notes.[7]
Comparison of Cancer Incidence Rate with other Cancer Registries of NCDIR and TMH rural registries.
[Figure 3] shows the comparison of Cancer Incidence Rate (per 100,000) with other NCDIR Cancer Registries, TMH rural registries and CI-5 Vol. XI registries.[2,7-10] The rates in Ratnagiri district is much lower than the international rates and also other Indian registries. [Figure 3] shows the higher rates in France, Bas-Rhin in male and USA Connecticut in female. The rates are lower in Sindhudurg for both male and female.

- Comparison of AAR (per 100,000) of Ratnagiri registry (2015–2016) with other registries.
Comparison of mouth cancer is shown in [Figure 4].[2,7,8] It is seen that mouth cancer rate in Ratnagiri is higher than Barshi, Dindikal and Bangalore registry but lower than in Chennai, Mumbai and Ahmedabad Urban registries.
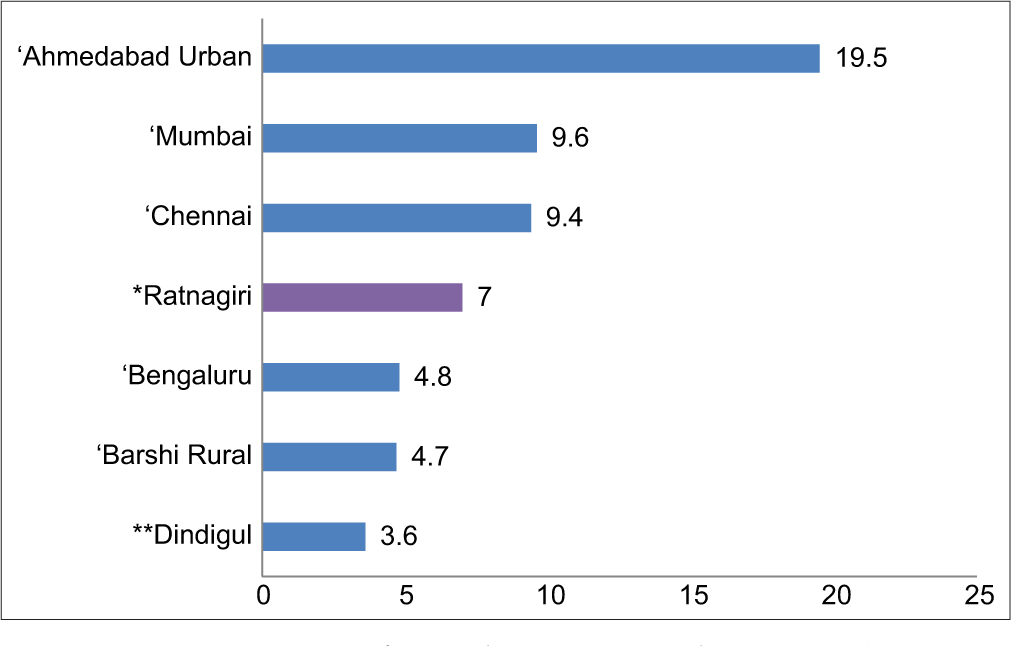
- Comparison of mouth cancer incidence rate (AAR per 100,000) of Ratnagiri with other NCDIR cancer registries – male.
In females, Breast Cancer is the leading site of cancer in breast cancer was the leading site of cancer in Ratnagiri District. [Figure 5] shows the comparison of breast cancer incidence rate with other NCDIR cancer registries[2,7,8] Breast cancer rate in Ratnagiri is lowest as compared to other NCDIR registries.
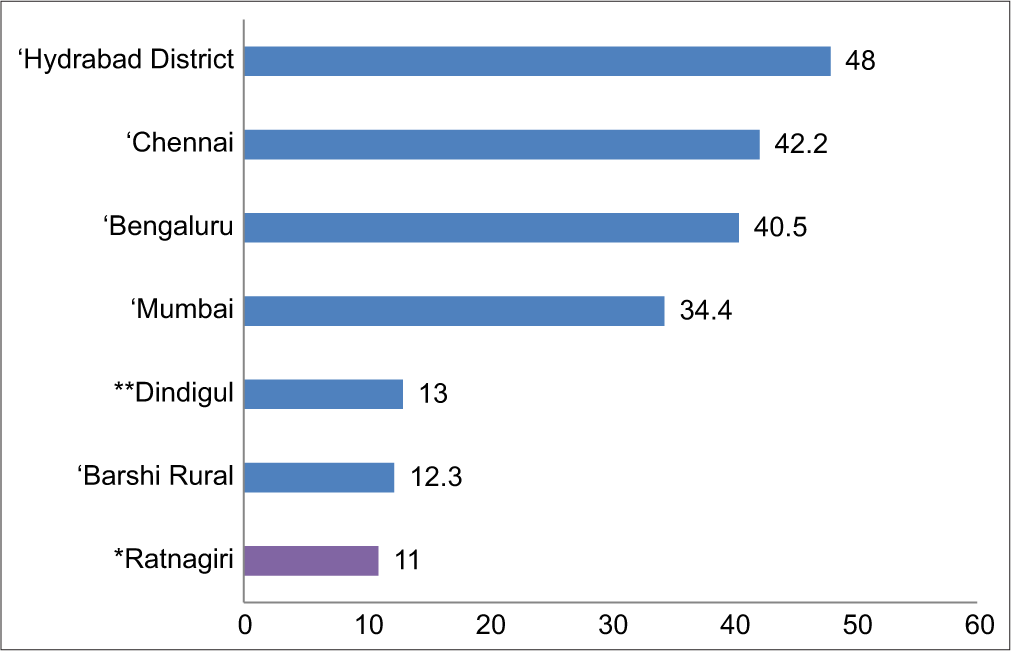
- Comparison of breast cancer incidence rate (AAR per 100,000) of Ratnagiri with other NCDIR cancer registries – female.
DISCUSSION
It is reported that 75–80% of patients have advanced disease (stage 3–4) at the time of diagnosis in India, possibly due to low level of awareness or education in the population and also lack of facilities in local areas, long distance to travel to reach tertiary cancer center and financial constraints contributes to the late diagnosis.[11,12] Government of India has been taking effort to establish regional cancer centers in rural areas for the early detection and treatment.
According to 2011 census data, 84% of the population of Ratnagiri district live in rural part of District and 16% resides in Urban areas. Furthermore, there was no major cancer hospital in Ratnagiri district, until 2003. B.K.L. Walawalkar hospital, a General hospital in Dervan was developed into a comprehensive cancer care center with the help of TMC, Mumbai.
TMC started the population-based cancer registry in Ratnagiri district to assist the existing cancer screening activity in 2009. The project has an excellent potential for community-based epidemiological study to identify the risk factors.
According to Ratnagiri Cancer Registry report, the cancer incidence rate lies between 39 and 47 (age-adjusted incidence rate) per 100,000. The cancer rates in Ratnagiri District are comparable with other rural cancer registries in India.
As per NCDIR report, the incidence of cancer is low in rural India compared to urban India and the cancer pattern is different in rural India compared to Urban India.[13] Due to environmental, diet and lifestyle variations in different parts of country the leading sites also differ in region accordingly. According to 2015–2016 report of Ratnagiri Cancer registry, mouth cancer is the leading site of cancer followed by Tongue in males. Furthermore, nearly 65% of cancer sites in male and 38% of cancer sites in female are associated with the use of tobacco.
In India, almost one-third of the cancers were known to be associated with the use of tobacco. Approximately, 70% of the Indian cancers (40% tobacco related, 20% infection related, and 10% others) are caused by potentially modifiable and preventable risk Factors.[14,15] As per NFH-5, in the year 2019–20, the tobacco consumption in rural Maharashtra was 38% in males and 6% in females; however, no data are available from Ratnagiri district, Maharashtra, on tobacco consumption.[16]
The consumption of tobacco is a major risk factor for cancers. The cancers of oral cavity, oropharynx, nasopharynx, hypopharynx, paranasal sinus, larynx, lung, esophagus, stomach, gall bladder, liver, pancreas, colon, rectum, kidney, ureter, renal pelvis, urinary bladder, and myeloid leukemia are related to tobacco use. However, these are preventable cancers and can be prevented through education and public awareness programs at various levels of the population.
Furthermore, the breast cancer as well as mouth cancer rates in Ratnagiri District among females are higher than the cervical cancer rates which are unlike of those observed in Indian rural registries (viz., Barshi). This probably is due to urbanized life style where breast cancer rates are more than the cervical cancers among females.
Cancer registration in India faces several challenges because it is not a notifiable disease, posing challenges to data collection and the mortality registration system has several gaps, including incomplete and inaccurate certification of cause of death.[14] Medical records are not properly maintained in many hospitals, low quality of medical notes add to the problem for the registry staff. Most of the time, the concerned registry staff has to go through all hospital records and death certificate to identify cancer cases as there is a lack of proper ICD-O[4] and ICD-10[5] coding in many hospitals.[1] Lack of information on the death certificate or poor death registration system is the major problem to identify the cause of death. It is necessary to improve the death registration system which includes the implementation of standard core information mortality form in all hospitals, nursing homes in registration area and at birth and death registration units of the vital statistics department and at burial grounds and crematoriums.[17] Furthermore, due to hilly areas, access to this area is not easy. The terrains are very steep and not easily reachable.
PBCRs can serve to identify possible causes of cancer in the community and to assess the impact of cancer control activities.[18] This study provides a framework for assessing the burden and trends of cancer in Ratnagiri district. Furthermore, the Jaitapur nuclear power plant (NPP) is an upcoming project in Ratnagiri district as proposed by Government of India. This will help to assess the incidence of cancer in the vicinity of power plant. Thus, it will be worthwhile to see the cancer incidence post-NPP commissioning in Ratnagiri district.
Cancer control activities
It is evident that tobacco consumption is high in rural area and Ratnagiri district is no exception. In fact, the overall tobacco consumption is 44% in Maharashtra, and average in India is 45%. TMH has conducted a vast screening program in Ratnagiri district for common cancers. Since 64.1% in males and 37.9% in females are tobacco-related cancers (TRC), prevention is a big challenge to reduce the TRC and being a lifestyle pattern, it can be modified for reducing the morbidity and mortality. BKL Walawalkar hospital in Dervan, Ratnagiri is a comprehensive cancer center, the hospital can take initiative for large scale awareness and prevention activities. The outcome of the awareness will be seen after a decade or so, especially with legislation by Government of India.
CONCLUSION
Cancer registry is difficult preposition to establish and function especially in developing countries which lack the required infrastructure and resources. Specialists from TMC and Walawalkar Hospital are putting their efforts for prevention, early diagnosis, and treatment through various cancer control activities in this district. The registry outputs are vital and important in view of developing the cancer control programs in this district and the information obtained shows the clear indication of the burden of cancer.
Acknowledgment
I am thankful to the Director. I would also like to thank all the Ratnagiri Registry Staff.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Tata Memorial Centre , Mumbai India.
References
- Population based cancer registry of India-the challenges and opportunities. Asian Pac J Cancer Prev. 2018;19:2885-9.
- [Google Scholar]
- Report of National Cancer Registry Programme (2012-2016) 2020. Available from: https://www.ncdirindia.org/all_reports/report_2020 [Last accessed on 2021 Jan 15]
- [Google Scholar]
- Office of the Registrar General and Census Commissioner, India. Available from: https://censusindia.gov.in/2011census/dchb/dchb_a/27/2732_part_a_dchb_ratnagiri.pdf [Last accessed on 2021 Jan 28]
- [Google Scholar]
- International Classification of Diseases for Oncology (3rd ed). Geneva: World Health Organization; 2000.
- [Google Scholar]
- ICD-10, International Statistical Classification of Diseases and Related Health Problems Geneva: World Health Organization; 2019.
- [Google Scholar]
- SPSS-statistical Package for the Social Sciences for Windows, Version 21.0 Armonk: International Business Machines; 2012.
- [Google Scholar]
- TMC-DAE Network of Cancer Registries, Ratnagiri Population based Cancer Registry Report 2015-16: 2020
- [Google Scholar]
- Cancer Incidence in Five Continents Volume XI. 2017. France: International Agency for Research on Cancer; Available from: https://ci5.iarc.fr [Last accessed on 2021 Jan 15]
- [Google Scholar]
- TMC-DAE Network of Cancer Registries, Sindhudurg Population based Cancer Registry Report 2015-16: 2021
- [Google Scholar]
- TMC-DAE Network of Cancer Registries, Visakhapatnam Population based Cancer Registry Report 2015-16: 2020
- [Google Scholar]
- The growing burden of cancer in India: Epidemiology and social context –. [Pubmed] Available from: https://pubmed.ncbi.nlm.nih.gov/24731885 [Last accessed on 2021 Jan 28]
- [Google Scholar]
- Radiation oncology in India: Challenges and opportunities. Semin Radiat Oncol. 2017;27:158-63.
- [CrossRef] [PubMed] [Google Scholar]
- National Cancer Registry Programme, Indian Council of Medical Research: Three Year Report of Population Based and Hospital Cancer Registries. 2012-14. Available from: https://www.ncdirindia.org [Last accessed on 2021 Jan 28]
- [Google Scholar]
- Cancer statistics, 2020: Report from National Cancer Registry Programme, India. JCO Glob Oncol. 2020;6:1063-75.
- [CrossRef] [PubMed] [Google Scholar]
- Burden of preventable cancers in India: Time to strike the cancer epidemic. J Egypt Natl Canc Inst. 2017;29:11-8.
- [CrossRef] [PubMed] [Google Scholar]
- National Family Health Survey (NFHS-5), India, 2019-21: Maharashtra Mumbai: IIPS; 2021. p. :166.
- [Google Scholar]
- Role of the cancer registries in determining cancer mortality in Asia. Radiol Oncol. 2007;41:183-7.
- [CrossRef] [Google Scholar]
- Planning and Developing Population-based Cancer Registration in Low-or Middle-income Settings Lyon: IARC Technical Publication; 2015.
- [Google Scholar]




