
Translate this page into:
Psychological distress levels in patients of total knee arthroplasty and their adherence to home exercise program – A correlational study
*Corresponding author: Siddhanth Sunil Sawant, Department of Physiotherapy, Sancheti Institute, College of Physiotherapy, Sancheti Healthcare Academy, Pune, Maharashtra, India. thesis.siddhanth@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Parekh NM, Sawant SS, Dabadghav R, Shyam A, Sancheti PK. Psychological distress levels in patients of total knee arthroplasty and their adherence to home exercise program – A correlational study. Indian J Med Sci 2023;75:63-7.
Abstract
Objectives:
Older people commonly experience life stressors such as reduced mobility, chronic pain, and fatigue. This leads to loneliness, isolation, and psychological distress among them, putting them at risk of developing mental and psychological disorders such as depression, dementia and anxiety. In older people, total knee arthroplasty (TKA) is one of the most common orthopedic surgeries undertaken. For physical therapeutic rehabilitation, home exercise programs (HEPs) are prescribed post-surgery. These programs require a lot of self-motivation which is reduced in those with mental illnesses. The objectives of this study were to assess the psychological distress levels in patients, to assess their HEP adherence, and, lastly, to study whether there is a correlation between the patient’s psychological distress levels and their HEP adherence.
Material and Methods:
Forty-three subjects who underwent TKA were recruited during their post-operative hospital stay. Their demographic data and date of surgery were collected. At 1 month postoperatively, they were sent a Google form comprising two questionnaires-subsection B of the exercise adherence rating scale and patient health questionnaire-4 to measure adherence to HEP and psychological distress levels. Obtained scores were correlated using Spearman’s test. The confidence interval and P value were set at 95% and <0.05, respectively.
Results:
The mean age of the 43 subjects was 62.58 ± 9.15. Spearman’s correlation coefficient (r) was −0.47, that is, a moderate negative correlation was found and the P value obtained was 0.02 which is statistically significant.
Conclusion:
Psychological distress levels have a negative correlation with HEP adherence in patients with TKA.
Keywords
Depression
Distress
Exercise program
Compliance
Total knee replacement

INTRODUCTION
The World Health Organization’s definition of good mental health states: “It is a state of well-being in which the individual realizes his or her abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community.”[1] Good mental health provides people with the skills and resilience to face and deal with abnormal and potentially destructive stressors.[2] As we age, our lives involve several developmental gains and losses.[3] Research shows an age-related increase in the amount of chronic and less controllable stressors such as reduced mobility, chronic pain, hearing loss, and fatigue.[4,5] Older people (more than 60 years) experience events of bereavement, retirement, etc. This leads to them facing loneliness, isolation, and psychological distress.[6-8] Thus, many old people are at risk of developing mental and psychological disorders such as depression, dementia, and anxiety.[8-10]
In the same population, total knee arthroplasty (TKA) is one of the most common orthopedic surgeries performed. The causes are degenerative joint diseases like severe osteoarthritis (OA) for those with damaged joints due to septic arthritis or osteomyelitis, joint reconstruction post-trauma, etc.[11-13] Post-surgeries, physiotherapeutic rehabilitation is a requisite and has proven to show short-term benefits in pain levels, range of motion, and level of functioning.[14,15] Physical therapy is performed in hospitals, tertiary care centers such as outpatient departments, and in the form of home visits.[16]
A home exercise program (HEP) is a protocol of exercises, explained, and taught to the patients by a physical therapist. It includes the exercises to be done, their frequency, intensity, repetitions, and sets.[17] In rehabilitation after hospital discharge, the exercises are frequently prescribed multiple times a day. The HEP performed by the patient, without a professional’s supervision, is an important aspect of recovery post orthopedic surgeries.[18] Patients take physiotherapy sessions through outpatient appointments at tertiary healthcare centers or home visits by therapists and also have HEPs multiple times a day. These HEPs require a lot of motivation on the part of the patient. This motivation is reduced in those living with mental illness.[19]
In some scenarios, despite the therapist ensuring complete treatment of the patients at a rehabilitation center or at their home, the patient is unable to adhere to their HEP. If the underlying cause for this is a mental health condition, then it has to be identified using screening tools and then tackled appropriately.[19] Post-TKA, if patients’ adherence to the HEP is subpar, it might result in an outcome that is inadequate to what is expected in healthier scenarios. A person’s mental health affects their pharmacological medical treatment adherence. The effect of psychological distress on their prescribed exercise adherence is yet to be seen.[20] The study hypothesis is that there is a negative correlation between a patient’s psychological distress levels and their adherence to HEP.
MATERIALS AND METHODS
The study was approved by the Institutional Ethical Committee before beginning and it was conducted in accordance with the guidelines of the Declaration of Helsinki.
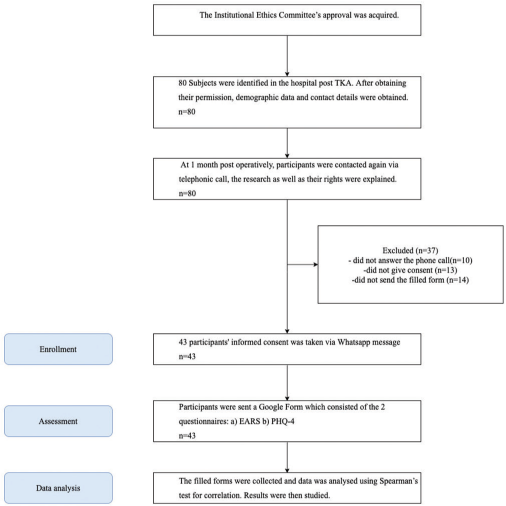
This was an observational cross-sectional study. It was conducted over a span of 6 months. The sample size was calculated using the G-power Software. The confidence interval was set at 95%. Convenience sampling was done and 80 eligible participants were identified from a tertiary care setup. At the set-up, males and females who could comprehend English and had undergone unilateral or bilateral TKA were included in the study. Patients who had any fractures of limbs or the spine were excluded from the study.
A verbal explanation of the study was given to the 80 identified participants during their immediate postoperative stay at the hospital. Verbal consent was taken from them and their demographic data, surgery undergone, date of surgery, and contact information was collected. At 1 month postoperatively, the participants were contacted by researchers through a telephone call. Informed consent was taken from 43 willing participants. Participants were then sent an online form that consisted of the two outcome measures used – part B of the exercise adherence rating scale (EARS) for exercise adherence and the patient health questionnaire-4 (PHQ-4) for psychological distress levels. The filled forms were then collected, and final EARS and PHQ-4 scores were calculated [Table 1].
 |
Outcome measures
For HEP exercise adherence
Part B of the EARS Newman-Beinart et al. developed the EARS since there is no gold standard for assessing exercise adherence behavior and there is a need for a valid and reliable tool to assess the same. The scale consists of six questions which are scored on a Likert scale. The final scores range from 0 to 24, with a higher score indicating better exercise adherence.[21]
For psychological distress levels
PHQ-4 This is an ultra-brief measure of depression and anxiety in the general population. The scale consists of four questions, scored on a Likert scale of 0–12. The first two questions screen for anxiety, while the next two screens for depression. Scores are rated as normal (0–2), mild (3–5), moderate (6–8), and severe (9–12). A total score ≥3 for the first two questions suggests anxiety. A total score ≥3 for the last two questions suggests depression.[22,23]
Statistical analysis
The age of the participants and the EARS and PHQ-4 scores was presented as mean ± standard deviation. These were calculated on Microsoft Excel for Windows. Correlation between the EARS and PHQ-4 scores was studied using Spearman’s test for correlation since both variables are non-parametric. Correlations were considered statistically significant at P < 0.05. All the statistical tests were done using SPSS version 21 for Windows.
RESULTS
Forty-three people participated in this study, of which 31 were female and 12 were male. The mean age of the participants was 62.58 ± 9.15 years. The mean ± standard deviations of the EARS scores were 18.63 ± 4.16 and the PHQ-4 scores were 2.44 ± 2.21. Spearman’s correlation coefficient (r) found is −0.47, that is, a moderate negative correlation is found between psychological distress levels and adherence to HEP. The P value obtained is 0.02, that is, it is a significant correlation [Figure 1].

- Correlation of patient health questionnaire-4 (PHQ-4) to exercise adherence rating scale (EARS) scores; x axis: PHQ-4 score and y axis: EARS score.
DISCUSSION
The study concluded that a negative correlation exists between psychological distress levels and adherence to HEPs, in patients of TKA. It was found that higher psychological distress levels were correlated with lower adherence to HEP in this study. This association between stress and exercise adherence has been previously reported by Stetson et al. in a study conducted on community-residing women. They looked at the effects of stress on exercise behavior in these women who were exercising on their own and found that in weeks with a high frequency of stressful events, participants exercised less and reported lesser self-efficacy for meeting upcoming exercise goals.[24]
These results support those found in Da Silva et al.’s research in which they studied 9309 participants for data on physical activity, anxiety, and depression and ten other covariates. This study showed that patients who showed symptoms of anxiety and depression had higher chances of not meeting the recommended levels of physical activity.[25] The probable cause for this behavior could be the time since which the patient has been physically active. Such as habituated exercisers become more active in the face of stress while those starting out might fall off track. The authors of this study suspect that their results support the aforementioned studies due to the population consisting of 72.09% women. Depression symptoms were shown to disproportionately affect women and older people, as seen in Sale et al.’s cross-sectional cohort study.[26]
Another factor for those with higher psychological distress could be the presence of chronic persistent pain even post-surgery. Chodór and Kruczyński’s study shows that female gender, psychological distress, and severity of acute postoperative pain were the risk factors for chronic persistent pain after TKA.[27] Hanusch BC et al. investigated the impact of comorbidities on pain persisting 2 and 5 years after surgery. Among the numerous ailments reported, only anxiety and depression were shown to increase the risk of developing chronic post-surgical pain after TKA. Pre-operative thoughts affect post-surgery distress and function seen weeks later.[28] These possibly aggravated the psychological distress levels and led to difficulty in performing the exercises.
Eight studies in a systematic search by Stults-Kolehmainen and Sinha showed marginal or no correlation between distress levels and adherence.[29] The cause for our study has found a negative correlation is suggested to be due to the choice of reliable outcome measures used for the two variables. OA, a progressive disease, is one of the causes of people undergoing TKA. Patients awaiting surgery can experience anxiety. While surgery does improve the quality of life (QoL) of patients, patients with OA along with anxiety and depression may not experience similar favorable clinical outcomes following joint replacement surgery as seen in those with OA without these comorbidities, even after a structured rehabilitation program.[30,31]
The clinical application of this study is that patients should be screened for psychological distress after surgeries to identify those at a higher risk. Before being discharged from the hospital, patients should be counseled better about deteriorating mental health, signs to look out for, and seeking help from healthcare professionals immediately. Supporting the study by Lin, good depression care has far-sighted benefits beyond just the disease, especially in those with OA and comorbid depression. Holistic care can reduce pain, and improve functional status, and quality of life in patients.[32]
In the study by Lopez-Olivo, patients’ level of education, tangible support, depression, and dysfunctional coping were associated with pain and functional outcomes after knee replacement.[33]
The study provides valuable insights into the correlation between psychological distress levels and adherence to HEPs in patients with TKA. The authors have used a rigorous methodology and validated measures to assess the psychological distress levels and adherence to HEPs. The findings suggest that addressing the mental health concerns of patients undergoing TKA may improve their adherence to HEPs, which can lead to better outcomes for patients.
Furthermore, there are some other limitations that also need to be addressed. The study used convenience sampling, which may limit its generalizability to other populations. In addition, the impact of other factors such as social support or physical activity levels on adherence to HEPs was not assessed. As the correlation between the psychological distress levels and the adherence to the HEP was to be studied, the study did not look into the causes for the psychological distress, the patient’s levels of education or support system or exercise beliefs or coping strategies, and recognize it as a limitation. Therefore, future studies should consider using a diverse sample and assessing the impact of other factors on adherence.
Only English speaking population was considered as the questionnaires used were in English. Another limitation of the study was that since it was conducted over the Internet, a large number of people initially included in the study did not respond 1 month postoperatively and the resultant sample size of the study was small.[34]
Further, the scope of the study is as follows. Differences in psychological distress levels in those who have undergone unilateral versus bilateral TKA can be studied. The differences in the stress levels correlating to questions of anxiety and depression separately and their impact on adherence to HEP can be reviewed. The study can also be done in various surgeries other than TKA.
CONCLUSION
The study concluded that a negative correlation exists between psychological distress levels and adherence to HEPs, in patients of TKA. The patients of TKA with high psychological distress showed poor adherence to home exercise protocols.
Acknowledgment
The author is thankful for all the participants who participated and gave time for this study. The author would also like to acknowledge their teachers, classmates, friends, and family for all their help and guidance. Finally, the author would also like to thank Shruti Modi for their support.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Prevention of Mental Disorders: Effective Interventions and Policy Options: Summary Report/A Report of the World Health Organization Dept, of Mental Health and Substance Abuse; In Collaboration with the Prevention Research Centre of the Universities of Nijmegen and Maastricht. Available from: https://apps.who.int/iris/handle/10665/43027 [Last accessed on 2012 June 16]
- [Google Scholar]
- What is good mental health? A scoping review. Eur Neuropsychopharmacol. 2020;31:33-46.
- [CrossRef] [PubMed] [Google Scholar]
- Theoretical propositions of life-span developmental psychology: On the dynamics between growth and decline. Dev Psychol. 1987;23:611-26.
- [CrossRef] [Google Scholar]
- Association between speech and high-frequency hearing loss and depression, anxiety and stress in older adults. Maturitas. 2018;110:86-91.
- [CrossRef] [PubMed] [Google Scholar]
- Patients who consult with tiredness: Frequency of consultation, perceived causes of tiredness and its association with psychological distress. Br J Gen Pract. 1994;44:413-6.
- [Google Scholar]
- Retirement and mental health: Does social participation mitigate the association? A fixed-effects longitudinal analysis. BMC Public Health. 2017;17:526.
- [CrossRef] [PubMed] [Google Scholar]
- Does believing in “use it or lose it” relate to self-rated memory control, strategy use, and recall? Int J Aging Hum Dev. 2010;70:61-87.
- [CrossRef] [PubMed] [Google Scholar]
- Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychol Aging. 2006;21:140-51.
- [CrossRef] [PubMed] [Google Scholar]
- Perceived distress and its association with depression and anxiety in breast cancer patients. PLoS One. 2017;12:e0172975.
- [CrossRef] [PubMed] [Google Scholar]
- Total knee arthroplasty after prior bone or joint sepsis about the knee. Clin Orthop Relat Res. 2002;404:226-31.
- [CrossRef] [PubMed] [Google Scholar]
- Knee joint replacement as primary treatment for proximal tibial fractures: Analysis of clinical results of twenty-two patients with mean follow-up of nineteen months. Int Orthop. 2020;44:85-93.
- [CrossRef] [PubMed] [Google Scholar]
- Physical exercise after knee arthroplasty: A systematic review of controlled trials. Eur J Phys Rehabil Med. 2013;49:877-92.
- [Google Scholar]
- Effectiveness of physiotherapy exercise after knee arthroplasty for osteoarthritis: Systematic review and meta-analysis of randomised controlled trials. BMJ. 2007;335:812.
- [CrossRef] [PubMed] [Google Scholar]
- Physical therapy in the 21st century (Part II): Evidence-based practice within the context of evidence-informed practice. Physiother Theory Pract. 2009;25:354-68.
- [CrossRef] [PubMed] [Google Scholar]
- ACSM's guidelines for exercise testing and prescription 9th ed. 2014. J Can Chiropr Assoc. 2014;58:328.
- [Google Scholar]
- Home based exercise therapy for older patients with knee osteoarthritis: A randomized clinical trial. J Rheumatol. 2000;27:2215-21.
- [Google Scholar]
- Motivation and cognitive control in depression. Neurosci Biobehav Rev. 2019;102:371-81.
- [CrossRef] [PubMed] [Google Scholar]
- Adherence to Exercise Scale for Older Patients (AESOP): A measure for predicting exercise adherence in older adults after discharge from home health physical therapy. J Geriatr Phys Ther. 2007;30:69-78.
- [CrossRef] [PubMed] [Google Scholar]
- The development and initial psychometric evaluation of a measure assessing adherence to prescribed exercise: The Exercise Adherence Rating Scale (EARS) Physiotherapy. 2017;103:180-5.
- [CrossRef] [PubMed] [Google Scholar]
- An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics. 2009;50:613-21.
- [CrossRef] [PubMed] [Google Scholar]
- A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122:86-95.
- [CrossRef] [PubMed] [Google Scholar]
- Prospective evaluation of the effects of stress on exercise adherence in community-residing women. Health Psychol. 1997;16:515-20.
- [CrossRef] [PubMed] [Google Scholar]
- Bidirectional association between physical activity and symptoms of anxiety and depression: The Whitehall II study. Eur J Epidemiol. 2012;27:537-46.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between disease symptoms, life events, coping and treatment, and depression among older adults with osteoarthritis. J Rheumatol. 2008;35:335-42.
- [Google Scholar]
- Predicting persistent unclear pain following primary total knee arthroplasty. Ortop Traumatol Rehabil. 2016;18:527-36.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of psychological distress and perceptions of illness on recovery from total knee replacement. Bone Joint J. 2014;96:210-6.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of stress on physical activity and exercise. Sports Med. 2014;44:81-121.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of acute postsurgical pain and anxiety following primary total hip and knee arthroplasty. J Pain. 2013;14:502-15.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of psychopathology on patient-perceived outcomes of total knee arthroplasty within an indigent population. J Bone Joint Surg Am. 2012;94:e84.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of improving depression care on pain and functional outcomes among older adults with arthritis: A randomized controlled trial. JAMA. 2003;290:2428-9.
- [CrossRef] [PubMed] [Google Scholar]
- Psychosocial determinants of outcomes in knee replacement. Ann Rheum Dis. 2011;70:1775-81.
- [CrossRef] [PubMed] [Google Scholar]
- Participant dropout as a function of survey length in internet-mediated university studies: Implications for study design and voluntary participation in psychological research. Cyberpsychol Behav Soc Netw. 2010;13:697-700.
- [CrossRef] [PubMed] [Google Scholar]




