
Translate this page into:
Challenges and navigating conundrums in setting up an obstetrics and gynecology coronavirus disease facility in a pre-existing tertiary care hospital – An Indian perspective
 , Chetna Arvind Sethi2, Sangeeta Gupta1, Krishna Agarwal1, Nalini Bala Pandey2, Asmita Muthal Rathore1
, Chetna Arvind Sethi2, Sangeeta Gupta1, Krishna Agarwal1, Nalini Bala Pandey2, Asmita Muthal Rathore1

*Corresponding author: Niharika Dhiman, Department of Obstetrics and Gynecology, Maulana Azad Medical College and Associated Lok Nayak Hospital, New Delhi, India. nitti929@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dhiman N, Sethi CA, Gupta S, Agarwal K, Pandey NB, Rathore AM. Challenges and navigating conundrums in setting up an obstetrics and gynecology coronavirus disease facility in a pre-existing tertiary care hospital – An Indian perspective. Indian J Med Sci 2021;73(1):57-60.
Abstract
India at present has 145,779 active coronavirus disease (COVID) cases and 8884 deaths. Being the largest tertiary care health facility under Delhi Government, our center was designated as a 2000 bedded dedicated COVID hospital. In addition to establishing areas for COVID management, COVID Obstetrics and Gynecology area requires a dedicated set up for delivering women, an operating room, and a neonatal care unit. A phased evacuation plan begins by curtailing non-emergency services and postponing elective surgeries, this process may take longer for obstetrics than other specialties on account of labor and postnatal care. The percentage reduction in the number of elective obstetric and gynecological surgeries was 73% and further fell by 98% (n = 4; category C, D) over a period of 1 month of the evacuation phase, whereas the reduction in emergency cases was only 15% (n = 200) in the beginning and fell to 89%. During the surge phase of COVID, we were able to increase the inpatient surge capacity by 8% (n = 100) as the bed occupancy increased exponentially from 30% to 88%. The start of evacuation of the facility until the endpoint of the surge marks the most dynamic phase of establishing a COVID facility during a pandemic. Pre-event planning for surge capacity at the inception of such pandemics should be based on the local and regional policies which depend on the competing demands of resources to maintain sustainability. These logistical demands are dynamic and vary as the pandemic progresses through its phases.
Keywords
Surge capacity
Pandemics
Coronavirus disease 2019
Women’s Health
Tertiary Health Center

INTRODUCTION
The coronavirus disease 2019 (COVID-19) infection is an ongoing pandemic,[1] and the first case in national capital Delhi was reported on March 2, 2020. By June 13, Delhi reported 36824 cases with1214 deaths.[2] Being the largest tertiary health-care facility under Delhi Government, our center was designated as a 2000 bedded dedicated COVID hospital.[3]
We, hereby, discuss the dynamics of converting an existing OBG facility to a COVID set up, which involves a continuous change in logistical variables paralleling the phases of a pandemic.
The key logistical requirements include formulation of standard operating procedures (SOPs), infrastructure development, building surge capacity, maintaining supplies, and workforce management. This task was undertaken by a multidisciplinary team of obstetricians, anesthesiologists, pediatricians, and the Hospital Infection Control Committee (HICC).
FORMULATING SOPS
High quality of SOPs based on ethical principles, guided by procedural values, has a direct impact on preparedness and level of performance of a health-care facility.[4]
Department protocols were formulated as per available guidelines.[5-7] With a rapidly changing scenario of COVID-19, needs evolved fast over a period of 3-4 weeks, and we revised our SOPs thrice.
INFRASTRUCTURE EVALUATION AND ESTABLISHMENT
For conversion of the maternity block to a dedicated COVID OBG facility, reassignment of areas was done broadly into green and red zones aiming to create a facility safe for patients and health care workers (HCWs).
Blueprint of the floor plan made and dry run done before the facility was made functional. Pre-event planning was done to identify areas for surge capacity and floor plan was kept flexible.
EVACUATION OF PATIENTS FROM THE EXISTING FACILITY
In the emergent situation of rising COVID cases, footfall in OPD fell by 90%, followed by the curtailment of OPD services by the end of March.
Non-COVID inpatients were evacuated in a stratified manner over 2–3 weeks. Depending on the potential impact on inpatient surge capacity by cancelling or delaying surgery, gynecological cases with surgical intervention were categorized as those in which procedure: (a) has no impact; (b) can be delayed indefinitely; (c) can be delayed by a week; and (d) cannot be delayed.[8,9] Category A and B were discharged. Non-COVID tertiary care centers were identified and collaborated with, for the transfer of Category C. Category D was operated over the next few days and discharged.
The percentage reduction in elective obstetric and gynecological surgeries from February (n = 180) to March (n = 50) was 73% and further fell by 98% (n = 4; category C, D) in early April. The reduction in emergency cases (Category D) was only 15% (n = 200] from February to March and fell by 89% in April [Figure 1a].

- Evacuation Phase: (a) Staged reduction of non-COVID surgeries. (b) Step-wise evacuation of non-COVID patients.
The obstetric bed occupancy (n = 206) reduced to 23% in 1st week to 9% in 2nd week of evacuation, whereas the bed occupancy of gynecological patients (n = 72) reduced from 16% to 5%, respectively [Figure 1b].
SUPPLIES
A dedicated team managed the constant availability of patient care equipment and other supplies. Potential stockpiling was maintained to keep an adequate amount in reserve.
WORKFORCE DISTRIBUTION
Workforce assignment was guided by anticipated inpatient workload and bed occupancy – in labor and non-laboring areas while minimalizing exposure of HCWs.
Redeployment of workforce
The workforce from all the wards was pooled. Dedicated teams were deployed in different COVID areas. Each team worked for a period of 2 weeks, including residents, nursing staff, and paramedical workers guided by a lead consultant.[9]
Care and training of HCW
Regular training in infection prevention and control was taken by the HICC. The content of training was structured according to the guidelines on prevention and control of COVID infections in hospitals.[6,10]
Appropriate accommodation and transport arrangements were made, adequate quarantine, and testing ensured and constant psychological support was extended to HCWs through continuous motivation and appreciation.
DYNAMICS OF WORKFORCE AND PATIENT INFLUX
Each health-care facility must evaluate and plan for surge capacity and elevate to meet the challenging demands during such pandemics. Surge capacity has been defined as “ability to manage a sudden, unexpected increase in patient volume that would otherwise severely challenge or exceed the current capacity of the health-care system.”[11] The goal should be to increase the inpatient surge capacity between 10% and 20%, which may vary according to the resources available.[12] We managed to increase it by 8% (n = 100) as the bed occupancy increased exponentially from 30% in the 2nd week to 88% in the 5th week from of starting the COVID facility. The second week marked the initial phase of surge and additional sites of care outside the facility, COVID care/quarantine/isolation centers for mild cases were utilized. Admission dynamics changed over these few weeks; out of the total cases (n = 27) in the 2nd week 22% were positive and 78% were suspects, whereas in the 3rd week, the number of suspects decreased to 12% and positives cases increased to 88% (n=49) [Figure 2a]. With the rising number of patient admissions, the workfore was increased by 21% [Figure 2b].
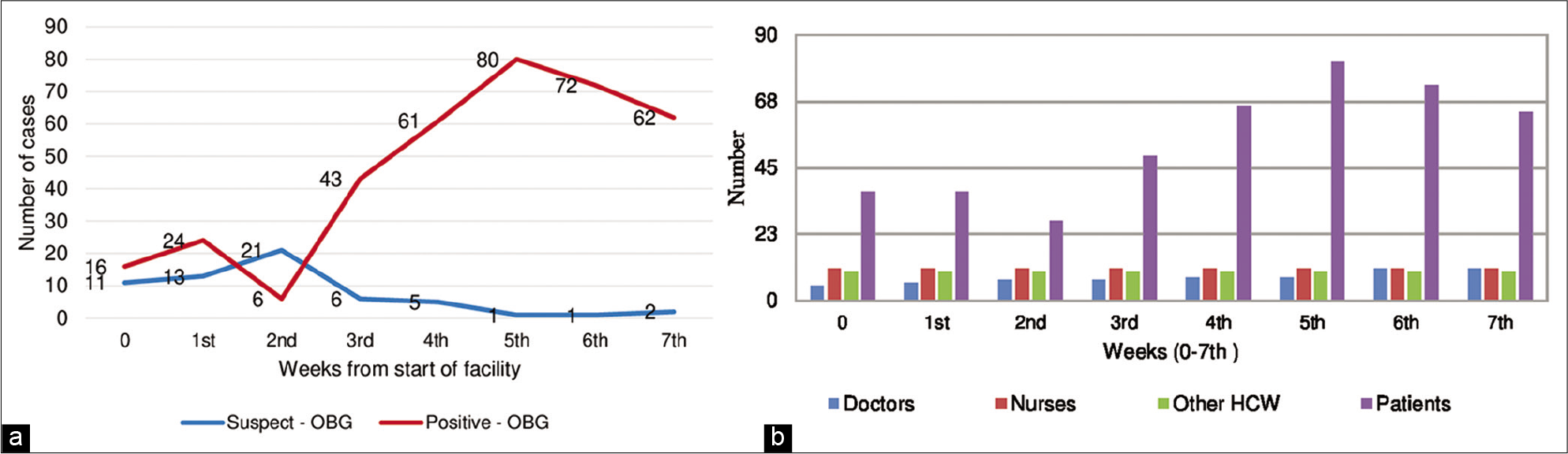
- Surge Phase: (a) Dynamics of influx of COVID patients for admission with respect to surge in disease. (b) Dynamics of workforce with increasing COVID patient influx.
We observed that from the beginning of evacuation until the endpoint of surge – a period of 5–6 weeks; marked the most dynamic phase of establishing COVID facility during the pandemic. This requires building of surge capacity with continuous modifications of its components – system, supplies, space, and staff.
CONSTRAINTS
Developing and operationalizing services to this unforeseen health-care emergency put the systems’ capacity to expand under enormous pressure. There was a single labor area for both suspects and confirmed cases; hence, individual labor suites were created, but the staff remained common. The preoccupation of the anesthesiologist in the care of sick and critically ill patients led to utilization of a dedicated operating room for COVID-19 patients common for all surgical specialties, in the intensive care unit block rather than in obstetrics and gynecology block.
Staff morale took an early hit due to multiple factors – fear and anxiety of getting infected, increasing workload due to implementation of strict infection control measures, and uncertainty over effectiveness and availability of personal protective equipment.
A subjective assessment of well-being of all the HCWs was done frequently. However, such assessments should be more objective and self-administered assessment tools for symptoms of depression PHQ-9 and Anxiety GAD-7 scale can be used.[13]
Regular assessment of dedicated COVID facilities should be done for their preparedness in preventing infection and promoting the satisfaction of HCWs.[14,15]
CONCLUSION
The preparedness of a health-care facility in the dynamic setting of evolving pandemic involves strategizing the management of infrastructure, workforce, and available resources. A phased evacuation plan begins by curtailing non-emergency services and postponing elective surgeries, this process may take longer for obstetric patients than others on account of labor and postnatal care. Pre-event planning for surge capacity should be made at the inception of such pandemics. The most dynamic phase of establishing COVID facility is from evacuation till the endpoint of surge, lasting for 5–6 weeks. The surge response should be based on the local and regional policies which depend on the competing demands of resources to maintain sustainability. These logistical demands are dynamic and vary as the pandemic progresses through its phases.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- WHO Director-General's Opening Remarks at the Media Briefing on COVID-19. 2020. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020 [Last accessed on 2020 Jun 12]
- [Google Scholar]
- COVID-19 Dashboard. 2020. Available from: https://www.mygov.in/COVID-19[Last accessed on 2020 Jun 13]
- [Google Scholar]
- Health and Family Welfare Department. 2020. Available from: http://www.web.delhi.gov.in/wps/wcm/connect/222c64804e1e41a8bfb8ffd194e333e1/GOVT+HOSP.pdf?MOD=AJPERES&lmod=-826499128&CACHEID=222c64804e1e41a8bfb8ffd194e333e1 [Last accessed on 2020 Sep 08]
- [Google Scholar]
- Ethics-based decision-making in a COVID-19 pandemic crisis. Indian J Med Sci. 2020;72:39-40.
- [CrossRef] [Google Scholar]
- Department of Health Research. 2020. Strategy of COVID-19 Testing in India. Available from: https://www.mohfw.gov.in/pdf/LabTestingAdvisory.pdf [Last accessed on 2020 Jun 12]
- [Google Scholar]
- Ministry of Health and Family Welfare. 2020. Directorate General of Health Services (EMR Division) Revised Guidelines on Clinical Management of COVID-19. Available from: https://www.mohfw.gov.in/pdf/RevisedNationalClinicalManagementGuidelineforCOVID1931032020.pdf [Last ac cessed on 2020 Jun 12]
- [Google Scholar]
- The Federation of Obstetric and Gynaecological Societies of India. 2020. Good Clinical Practice recommendation on Pregnancy with COVID-19 Infection. Available from: https://www.fogsi.org/the-draft-version-1-fogsi_gcpr_on_pregnancy_with_COVID_19_infection [Last accessed on 2020 Jun 12]
- [Google Scholar]
- Hospital emergency surge capacity: An empiric New York statewide study. Ann Emerg Med. 2007;50:314-9.
- [CrossRef] [PubMed] [Google Scholar]
- Coronavirus disease 2019 pandemic: Staged management of surgical services for gynecology and obstetrics. Am J Obstet Gynecol. 2020;223:85.
- [CrossRef] [PubMed] [Google Scholar]
- Infection Control Guidance for Healthcare Professionals about Coronavirus (COVID-19) 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control.html [Last accessed on 2020 Jun 13]
- [Google Scholar]
- Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004;44:253-61.
- [CrossRef] [PubMed] [Google Scholar]
- Hospital disaster preparedness in Italy: A preliminary study utilizing the World Health Organization hospital emergency response evaluation toolkit. Minerva Anestesiol. 2016;82:1259-66.
- [Google Scholar]
- Anxiety, depression and behavioural changes in junior doctors and medical students associated with the coronavirus pandemic: A cross-sectional survey. J Obstet Gynaecol India 2020:1-5.
- [CrossRef] [Google Scholar]
- COVID-19 health facility preparedness for protecting healthcare workers: Designing a tool for rapid self-assessment. Indian J Med Sci. 2020;72:83-7.
- [CrossRef] [Google Scholar]
- Ensuring safety and availability of healthcare workers in the era of COVID-19: An experience from the Eastern State of India. Indian J Med Sci. 2020;72:58-64.
- [CrossRef] [Google Scholar]




