
Translate this page into:
Difficult total thyroidectomy in radioiodine refractory Graves’ disease with pre-operative voice change

*Corresponding author: Sabaretnam Mayilvaganan, Department of Endocrine Surgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road, Lucknow - 226 014, Uttar Pradesh, India. drretnam@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mayilvaganan S, Mahalakshmi VD, Bhargav PR. Difficult total thyroidectomy in radioiodine refractory Graves’ disease with pre-operative voice change. Indian J Med Sci 2021;73(2):269-71.
Abstract
Thyroidectomy for Graves’ disease is challenging and if the patient had radioiodine ablation with its inflammatory changes which can make total thyroidectomy a herculean task. Here, we present a case of Graves’ disease with exophthalmos who underwent total thyroidectomy following 4 times radio ablation.
Keywords
Thyroidectomy
Graves’ disease
Voice change

INTRODUCTION
Voice change is regarded as unusual presentation of benign thyroid disease. Holl-Allen reported a pre-operative incidence of vocal cord palsy accompanying benign thyroid disease of 0.69% (eight out of 1156 patients).[1] Vocal cord paralysis has been reported in association with radioiodine therapy for thyrotoxicosis by Craswell[2] in 1972 with 5 mCi, Snyder in 1978 with 7.3 mCi,[3] and Coover in 1999 and 2000 with 29.3 mCi[4] with recovery of vocal cord paralysis after 3 weeks, 20 months, and no recovery by 14 months as reported. The patient we report here is of interest because of voice change associated with a benign diffuse toxic goiter and difficult thyroidectomy following four doses of radioiodine ablation.
CASE REPORT
A 46-year-old unmarried premenopausal lady headmistress by occupation presented with complaints of swelling in front of neck from 3 years which was gradual in onset, painless with progressive increase in size, and swelling of both legs from 1 month. She complained of change in voice from 1 year and protrusion of eyeballs from 4 years with frequent change in glasses from 1 year and watering of eyes from 6 months. She gave a history of palpitations and tremors from 25 years. On examination, she has exophthalmos [Figure 1], 10 cm × 6 cm thyroid swelling with nodular surface, variegated consistency. She had no cervical lymphadenopathy, but had fine tremors of hands and non-pitting edema of forearm and legs. Her thyroid profile was suggestive of suppressed thyroid-stimulating hormone (TSH) and elevated T3 and T4 and thyroid scan suggestive of diffuse toxic goiter with thyroid:parotid ratio (T:P) – 40:28, USG neck: s/o enlarged both lobes of thyroid with heteroechoic pattern and increased vascularity. CECT scan showed diffusely enlarged both lobes of thyroid with hypodense nodule of size 2 cm × 2 cm at inferior pole of the left lobe of thyroid [Figure 2]. Her pre-operative indirect laryngoscopy showed phonatory gap.

- Exophthalmos with goiter.
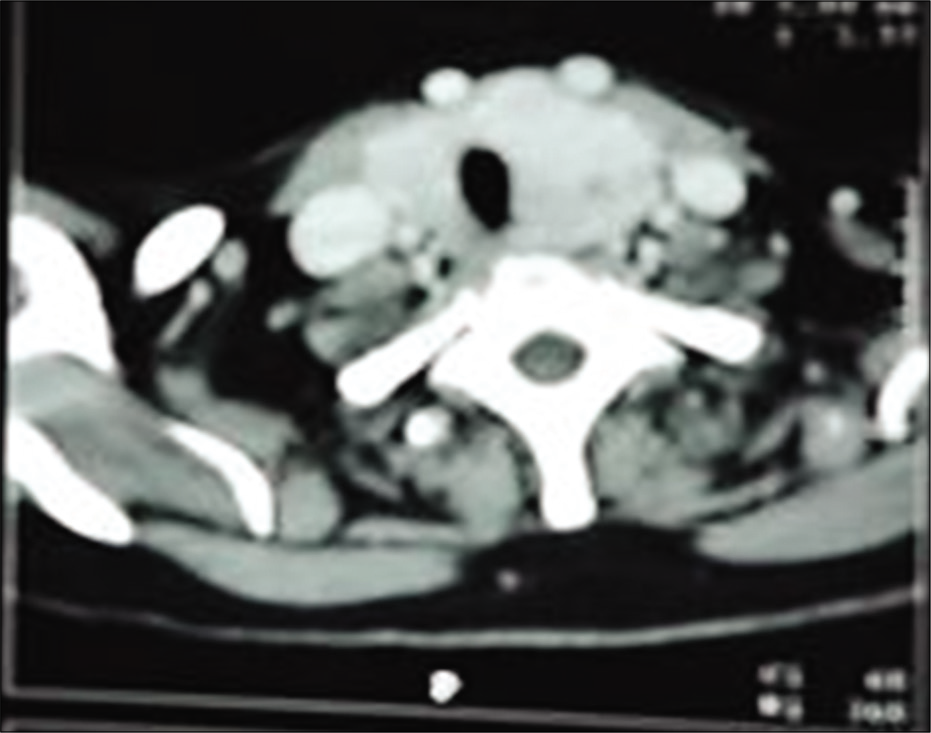
- CECT showing enlarged lobes.
She received antithyroid drugs for 6 months followed by radioiodine ablation 4 times, 3 monthly with doses of 8 mci, 10 mci, 12 mci, and 15 mci along with antithyroid drugs. Two months after two doses of radioiodine ablation, her TSH was high with 97 mIU with weight gain and coarse facies; hence, antithyroid medication was stopped. After 15 days of antithyroid drug withdrawal, she again presented with tremulousness and suppressed TSH with elevated T3, T4 following this episode, two more doses of radioiodine were administered at 3 monthly interval with higher doses along with antithyroid drugs. On follow-up after 2 months with no significant improvement in symptoms and elevated T3, T4 with suppressed TSH, the patient was referred for surgery on antithyroid drugs. Preoperatively, colossal iodine was given for 5–6 days along with carbimazole 10 mg TDS and propranolol 40 mg BD. She underwent uneventful total thyroidectomy with autotransplantation of both inferior parathyroids [Figure 3]. Her thyroidectomy difficulty scale was 15. Weight of the gland is 108 Gms and cut section shows multiple fleshy hard nodules with calcifications present in both lobes of thyroid. She developed biochemical and clinical hypocalcemia in the post-operative period and was managed with oral calcium and Vitamin D supplements. Final histopathology shows vague nodularity with lower pole of the left lobe showing foci of coagulative necrosis and features consistent with primary hyperplasia in resolution. Indirect Layngoscopy 6 weeks following Thyroidectomy showed normal vocal fold movement with normal voice.
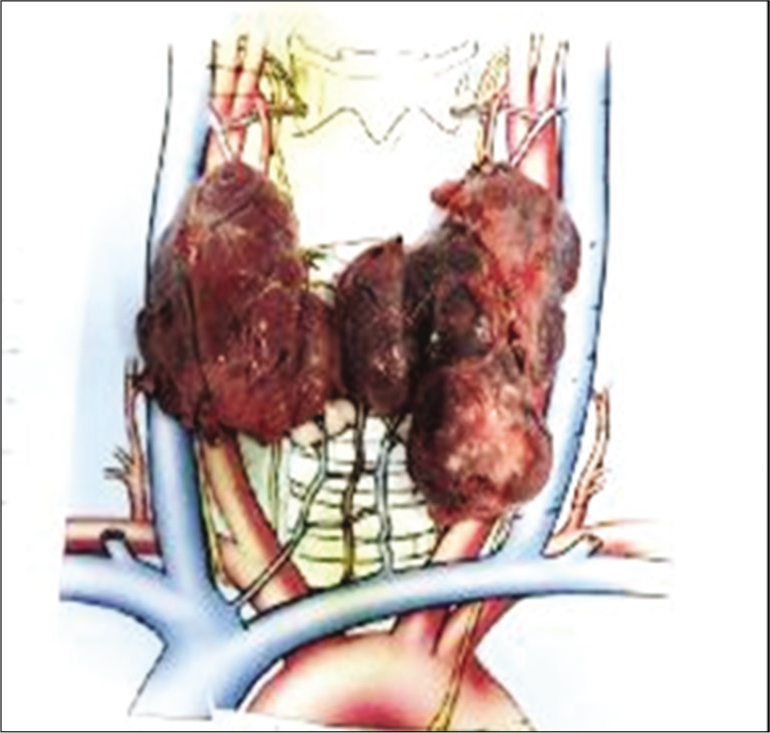
- Gross specimen.
DISCUSSION
Thyroidectomy for Graves’ disease is quite challenging with increased vascularity and high incidence of injury to parathyroids. Radioiodine ablation with its inflammatory changes can cause adhesions and make thyroidectomy more difficult. The surgeon has to carefully plan such surgeries and even might need to stage. The exposure has to be adequate and the dissection has to be meticulous for optimum results. We recommend ligation of both superior poles initially for adequate devascularization of the gland.
Although voice change with benign thyroid disease is unusual, cases have been reported. Laryngeal paralysis which may be reversible in most cases occurs rarely following radioiodine ablation.[4] This is a case of nodular Graves with ophthalmopathy and dermopathy with voice change and not responded to radioiodine ablation with a thyroidectomy difficulty score. Her pre-operative indirect laryngoscopy showed phonatory gap. Indirect laryngoscopy at 6 weeks post-operative was normal. Various mechanisms associated with vocal palsy in benign thyroid disease include compression of recurrent laryngeal nerve and/or its blood supply between goiter and c-spine or trachea, stretching of nerve, per nodular inflammation producing minute artery thrombosis and fibrosis involving nerve, and direct involvement in thyroiditis.
CONCLUSION
Large Graves’ disease which is not controlled by drugs and radioactive iodine shall be a difficult thyroidectomy and the endocrine surgeon should prepare such cases in good synchronization with the endocrinologists and also anesthesiologist.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Laryngeal nerve paralysis and benign thyroid disease. Arch Otolaryngol. 1967;85:335-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vocal cord paresis following radioactive iodine therapy. Br J Clin Pract. 1972;26:571-2.
- [Google Scholar]
- Vocal cord paralysis after I-131 therapy for solitary toxic nodule. J Nucl Med. 1999;40:505.
- [Google Scholar]




