
Translate this page into:
New secondary sign of ACL tear – The medial femoral notch sign (Gupta-Botchu sign)

*Corresponding author: Rajesh Botchu, Department of Musculoskeletal radiology, Royal Orthopedic Hospital, Bristol Road South, Birmingham - 312, United Kingdom. drbrajesh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Saad A, Almeer G, Azzopardi C, Gupta H, Botchu R. New secondary sign of ACL tear – The medial femoral notch sign (Gupta-Botchu sign). Indian J Med Sci 2021;73(1):124-6.
Abstract
ACL is the most common injured ligament of the knee. The diagnosis on MRI is by primary and secondary signs. We describe a new secondary sign of ACL tear – The medial femoral notch sign. (xxxxxx sign).
Keywords
Anterior cruciate ligament
Tear
Medial femoral notch sign

INTRODUCTION
The anterior cruciate ligament (ACL) is one of two major cruciate ligaments that aid in stabilizing the knee joint. It originates from the anteromedial aspect of the intercondylar zone of the tibial plateau inserting on the medial aspect of the lateral femoral condyle.[1] The ACL is the most commonly injured ligament of the knee joint.[2,3]
Although ACL injury can be clinically diagnosed, it may often pose a challenge to the clinician and MR imaging is often warranted to confirm the diagnosis.
On magnetic resonance imaging (MRI), ACL tears can be identified with “primary” and/or “secondary” signs.[4] Primary signs involve features directly related to the discontinuity of the fibers. Secondary signs include features due to sequelae of bony injuries (pivot shift pattern) related to the ACL, of which the lateral femoral notch sign (LFNS) is highly reliable. This is a distinct notch on the lateral femoral condyle, with a depth of approximately 1.5 mm or more.[5]
In this paper, we report an ACL tear with a medial femoral notch sign (MFNS-Gupta-Botchu sign) in a young patient, which has never been described in the literature. We discuss the possible biomechanics of MFNS.
CASE REPORT
We report a case of a 17-year-old boy who suffered a non-contact twisting-like injury to his right knee during a sporting activity. He noticed some knee instability when walking, warranting him to present to the clinic 4 weeks later. On examination, he exhibited a positive anterior drawer and Lachman’s test. Valgus and varus stress tests were negative. McMurray’s was mildly positive. This was investigated further with an MRI. The MRI demonstrated full-thickness tear of the ACL with marked anterior tibial translation [Figure 1]. The medial and lateral collateral ligament complex were intact. There was an undisplaced vertical tear of the periphery of the posterior horn of medial meniscus (RAMP). Lateral meniscus, posterolateral corner structures, and extensor mechanism were intact. There was no osseous edema. There was 3 mm focus of subchondral depression with a depth of 1 mm involving the mid-portion of the medial femoral condyle [Figures 2 and 3]. The overlying articular cartilage was intact. The lateral femoral condyle and proximal tibia had normal appearances. No fracture was demonstrated. He was managed surgically with an ACL reconstruction.
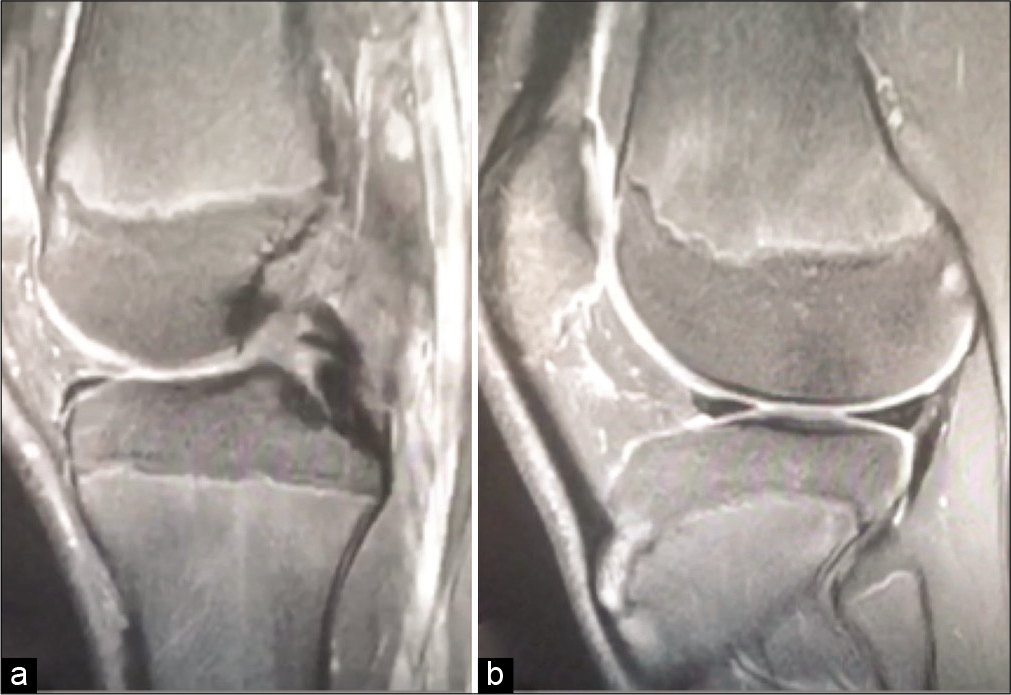
- Sagittal PDFS showing full-thickness rupture of the ACL (a) and anterior tibial translation (b).
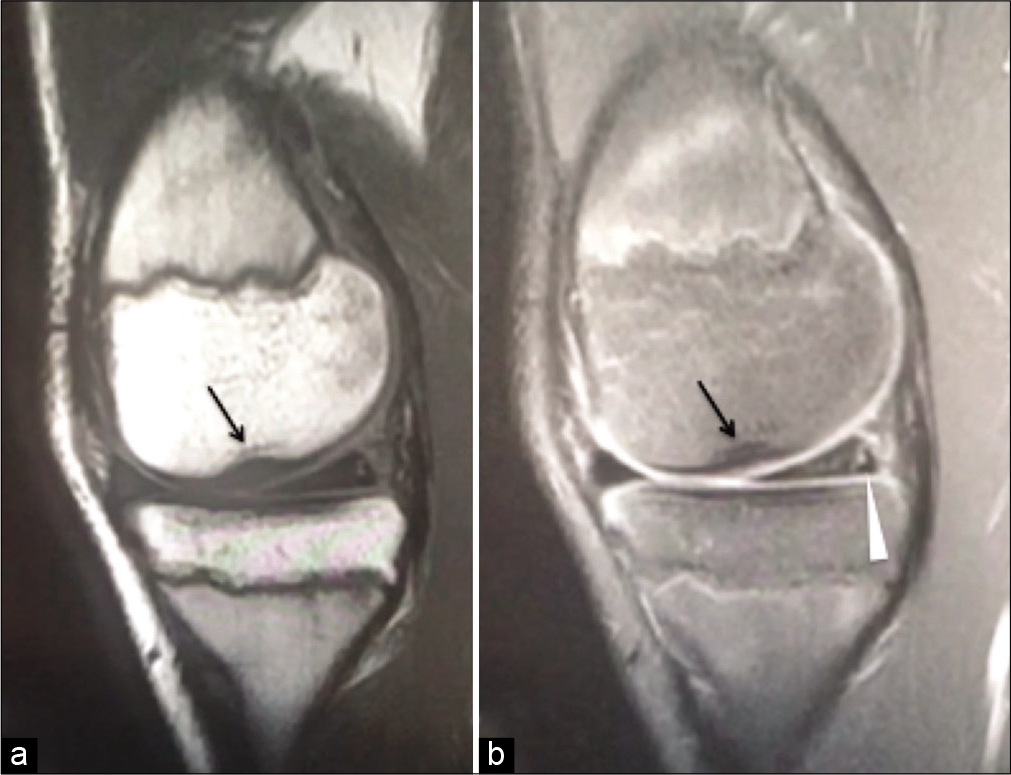
- Sagittal PD (a) and PDFS (b) showing medial femoral notch sign (Gupta-Botchu sign) (arrow) and tear of the medial meniscus (arrowhead).
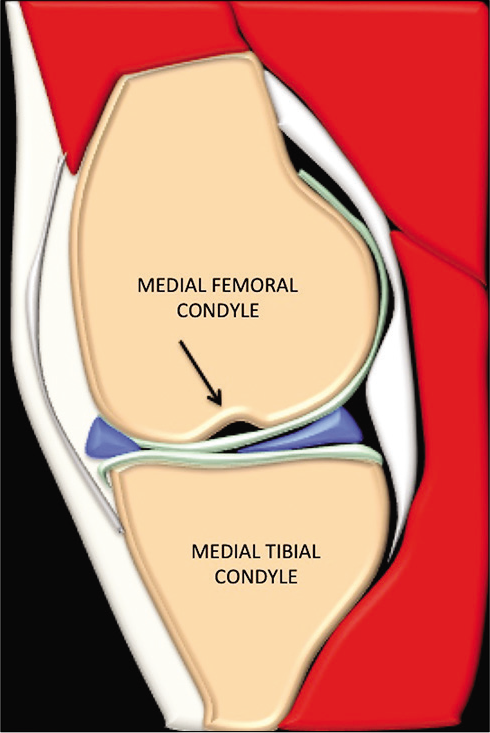
- Animation of the sagittal image of the knee through midmedial femoral condyle showing the medial femoral notch sign (Gupta-Botchu sign) (arrow).
DISCUSSION
ACL tears are common injuries, typically observed amongst young athletes, and sustained during sporting activities. The primary function of the ACL bundle is to limit the anterior translation of the tibia in relation to the femur and to counteract excessive external and internal rotation of the leg.[6] Injury to the ACL can, therefore, lead to serious instability of the knee joint. The mechanism of injury is complex but thought to involve anterior subluxation of the tibia in relation to the femur during a sudden change in direction of movement or high valgus stresses applied to the knee joint, with the ligament taught, while the tibia is in contact with the ground (pivot-shift).[6,7] This necessitates a large amount of force, which leads to injury of the other ligaments, including the medial or lateral meniscus and the medial collateral ligament, reported in up to 80% of all cases.[8]
ACL injuries can be diagnosed clinically, with highly specific tests which include anterior drawer (91% specificity), Lachman’s (94% specificity), and pivot-shift test (98% specificity).[2] MR is the primary imaging modality to confirm the diagnosis and decipher other ligamentous injuries, with a sensitivity of 86% and specificity of 95%, respectively.[2,4] The features of ACL tears can be defined on MRI as primary or secondary signs. Primary signs are due to loss of normal continuity of the ACL fibers or their osseous attachment and empty notch sign.
Secondary signs include anterior tibial translation of the tibia in relation to the femur (>7 mm), LFNS, straight LCL sign, lax patellar tendon, uncovering of the posterior horn of lateral meniscus, and buckling of PCL.
The LFNS, also known as the deep lateral condylar sulcus, is a highly reliable sign,[5,9] described as a depression of more than 1.5 mm deep, seen best on lateral radiographs or sagittal MRI and CT, in the lateral femoral condyle at the lateral condylopatellar sulcus. This is seen in 20–60% of ACL tears.[10,11] The depression occurs due to the impaction between the lateral femoral condyle and the posterolateral edge of the tibial plateau during the pivot shift pattern of injury.[6]
Our patient presented with an ACL rupture and a medial femoral condyle sulcus sign, an atypical finding that has never been described in the literature. There was no accompanying MCL, LCL, or posterolateral corner injury. There was a tear of the posterior horn of medial meniscus (RAMP), which is associated with a pivot shift pattern of injury. We hypothesize that the mechanism of this injury to the ACL was different to conventionally described mechanism. We hypothesize that the mechanism of injury was internal rotation with knee in flexion without any valgus or varus force. This could have resulted in the impaction of the condylopatellar sulcus of the medial femoral condyle within the posterior cortex of the proximal tibia resulting in the MFNS. This is not a normal variant and the authors have never seen this in over 8 years of experience during, which they have seen several 100’s if not 1000’s of MRI of the knee with a sporting injury. The medial femoral notching is unlikely to be due to separate injury due to the location of the notching and pattern of associated injury. We acknowledge this is a solitary case however, given the above, we strongly believe that MFNS and ACL rupture are sequelae of the same injury.
CONCLUSION
We report and describe a rare radiological finding with an ACL tear, the Gupta-Botchu (MFCS) sign that has never been reported in the literature.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Is anterior cruciate ligament graft rupture (after successful anterior cruciate ligament reconstruction and return to sports) actually a graft failure or a re-injury? J Orthop Surg (Hong Kong). 2019;27:2309499019829625.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior Cruciate Ligament (ACL) Knee Injuries Treasure Island, FL: StatPearls; 2020.
- [Google Scholar]
- Epidemiology of sports injuries-25-year analysis of a sports orthopedic-traumatological outpatient clinic. Sports Injury Sports Damage. 1999;13:38-52.
- [Google Scholar]
- Segmentation of the lateral femoral notch sign with MRI using a new measurement technique. BMC Musculoskelet Disord. 2015;16:217.
- [CrossRef] [PubMed] [Google Scholar]
- The lateral notch sign associated with acute anterior cruciate ligament disruption. Am J Sports Med. 2000;28:68-73.
- [CrossRef] [PubMed] [Google Scholar]
- Bone signal abnormalities in the posterolateral tibia and lateral femoral condyle in complete tears of the anterior cruciate ligament: A specific sign? Radiology. 1992;182:221-4.
- [CrossRef] [PubMed] [Google Scholar]
- Occult osseous lesions documented by magnetic resonance imaging associated with anterior cruciate ligament ruptures. Arthroscopy. 1991;7:45-51.
- [CrossRef] [Google Scholar]
- Anterior cruciate ligament reconstruction and the long-term incidence of gonarthrosis. Sports Med. 1999;27:143-56.
- [CrossRef] [PubMed] [Google Scholar]
- Spectrum of injuries associated with paediatric ACL tears: An MRI pictorial review. Insights Imaging. 2013;4:273-85.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and location of bone bruises associated with anterior cruciate ligament injury and implications for mechanism of injury: A systematic review. Sports Med. 2014;44:281-93.
- [CrossRef] [PubMed] [Google Scholar]




